Abstract
Irritable bowel syndrome (IBS) is a chronic functional disorder characterised by abdominal pain and altered bowel habits. The most prevalent subtype is diarrhoea-predominant IBS (IBS-D). The combination of Bacillus subtilis HU58 and Heyndrickxia faecalis (formerly Bacillus coagulans) SC208 has previously exerted positive effects in people with antibiotic-associated diarrhoea and infective diarrhoea. The present multicentre study conducted in India aimed to evaluate the effectiveness and safety of the dual-strain probiotic in adults (18-65 years) with IBS-D. In this randomised, double-blind, placebo-controlled pilot study, 61 participants were recruited and assessed for changes in abdominal pain intensity (Numeric Rating Scale, NRS) and stool consistency (Bristol Stool Form Scale, BSFS) over a 4-week intervention period, with secondary outcomes including responder rates for IBS Global Assessment of Improvement (IBS-GAI) and perceived stress (Perceived Stress Scale, PSS). The probiotic group showed significantly higher overall responder rates for both abdominal pain and stool consistency (
The trial is registered at https://ctri.nic.in/Clinicaltrials (CTRI/2022/07/044154).
1 Introduction
The human gut microbiota is a community of trillions of microorganisms â mostly viruses, bacteriophages and bacteria, fungi and protozoa â which reside in the human gastrointestinal (GI) tract (Valdes et al., 2018). These organisms and their metabolites are key components of the intestinal ecosystem, influencing human health through modulation of immune, metabolic, neurobehavioral and digestive processes (Fusco et al., 2023). Throughout the lifespan, several factors including diet, lifestyle, mental state, environmental exposures and infection may impact the composition and diversity of the gut microbiota, leading to the symptomatic dysregulation of GI functions and development of functional GI disorders (FGID) (Wei et al., 2021). The burden of functional GI symptoms is well documented, correlating to medical comorbidities, increased global healthcare costs and impaired quality of life (Dawoodi et al., 2022; Sperber et al., 2021; Tielemans et al., 2013).
Irritable bowel syndrome (IBS) is a common FGID, characterised by recurrent abdominal pain and associated changes in stool consistency and frequency, with diarrhoea-predominant IBS (IBS-D) being the most prevalent subtype accounting for 31.5% of cases globally (Oka et al., 2020). The predominance of diarrhoea in individuals with IBS presents a significant burden, correlating to worse quality of life and greater interference in daily activities (Singh et al., 2015).
In addition to dietary, lifestyle and pharmaceutical interventions, probiotics are commonly used for the management of IBS symptoms with documented positive outcomes. Probiotics are known to influence mucosal immune pathways through their interaction with commensal and pathogenic microbes, the production of metabolites, such as short chain fatty acids (SCFA), and communication with host cells via biochemical signalling, leading to improvements in functional GI symptoms with the reduction of diarrhoea being one of the most widely recognised (Guarner, 2023).
Such probiotic effects are known to be strain-specific and may be compromised by issues relating to their viability during manufacturing, storage and shelf life, yet whilst spore-forming strains offer a potential advantage due to their superior resistance to harsh environmental conditions, their efficacy is less widely documented than non-spore-forming probiotics (Guarner, 2023). Among the most widely studied spore-formers are those belonging to the Bacillus genus. In previous clinical trials, B. coagulans MTCC 5856 was found to decrease diarrhoea, abdominal pain and bloating in adults with IBS-D (Majeed et al., 2016) while B. cereus A05 was shown to be more effective at reducing diarrhoea than dietary fibre supplementation in individuals receiving enteral nutrition (de Castro Soares et al., 2017).
In particular, strains belonging to B. subtilis and Heyndrickxia faecalis (formerly B. coagulans, later reclassified as Weizmannia coagulans) have long been recognised for their probiotic potential, being known to survive the digestive tract and germinate in the gut where they exert their positive health effects (Casula and Cutting, 2002; Cutting, 2011; Hong et al., 2005). Consequently, they have been used as probiotic ingredients in dietary supplements and foods for human and animal health for several years and listed as probiotics by the Food Safety and Standards Authority of India (2022). As such these organisms are of ongoing interest to researchers.
Recent studies have demonstrated beneficial effects of the combination of B. subtilis (HU58â¢) and Heyndrickxia faecalis (SC208â¢) in individuals with diarrhoea (Dhongade, 2022, Mehta, 2020a). The B. subtilis HU58 strain was first isolated from a faecal sample from a healthy individual (Hong et al., 2009a). It is a Gram-positive, rod-shaped, spore-forming, aerobic/facultative anaerobic bacterium that is resistant to gastric fluids, undergoes rapid sporulation, and can form biofilms (Permpoonpattana et al., 2012). It has been reported to increase levels of short chain fatty acids (SCFAs), the relative abundance of beneficial microbial families, and the microbial diversity in an in vitro model of the human GI tract (Marzorati et al., 2020). H. faecalis SC208 is a spore-forming probiotic strain isolated from soil, known to produce SCFAs and digestive enzymes (Hong et al., 2009a, Hong et al., 2009b). The most recent reclassification of strain SC208 to H. faecalis was based on whole genome pairwise average nucleotide identity (ANI) with type strain H. faecalis Marseille-P8953T (Narsing Rao et al., 2023). H. faecalis and W. coagulans are closely related species and their high genetic similarity have resulted in the reclassification of strains previously assigned to W. coagulans into H. faecalis. Due to this reclassification the species share a common history of use. The safety profiles of both strains have been confirmed by genome sequencing and in several clinical trials (Dhongade, 2022; Dound et al., 2017; Mehta, 2020a,b).
In combination, the beneficial effects of B. subtilis HU58 and H. faecalis SC208 on intestinal permeability and immune markers have been demonstrated using an in vitro gut model, the mucosal simulator of the human intestinal microbial ecosystem (M-SHIME®), and an in vitro inflammatory bowel disease-like Caco-2/THP1 co-culture model in both healthy and antibiotic-induced dysbiosis conditions (Marzorati et al., 2020). This combination of probiotic strains has also been found to normalise stool consistency and frequency and alleviate abdominal pain in adults with antibiotic-associated diarrhoea (Mehta, 2020a) and children with infective diarrhoea (Dhongade, 2022), suggesting their potential positive effects on symptoms of diarrhoea from other causes. However, the effects of these spore-forming probiotics in individuals with IBS-D have not previously been reported, warranting separate investigation.
This was the first randomised, double-blind, placebo-controlled pilot study conducted in India that aimed to investigate the effects of a spore-based probiotic supplement containing the HU58 and SC208 strains on diarrhoea, abdominal pain, gut microbiota diversity and SCFA production, in an IBS-D population.
2 Materials and methods
Study design
This randomised, double-blind, placebo-controlled, parallel-group, multicentre pilot study investigating the efficacy and safety of a 4-week intervention of the HU58 and SC208 strains in a population of adults with IBS-D (as defined by Rome IV criteria) was conducted from August 2022 to January 2023 at five clinical sites in India: Dr Sanjeev Khanna Clinic, Mumbai; Healing Hands Clinic, Pune; Mysore Medical College & Research Institute and associated hospitals, Mysore; Pimpri Chinchwad Municipal Corporationâs Post Graduate Institute (PCMCs PGI) Yashwantrao Chavan Memorial Hospital, Pune; and Saideep Healthcare & Research Centre, Ahmendnagar. Written favourable opinion for the conduct of the study was provided by V Care Independent Ethics Committee (7th July 2022, Reg. No ECR/334/Indt/MH/2020) for Dr. Sanjeev Khanna Clinic, and by the respective institutional ethics committees for Healing Hands Clinic (30th July 2022, Reg. No ECR/238/Indt/MH/2017/RR-21), Mysore Medical College & Research Institute (18th September 2022, Reg. No. ECR/134/Inst/KA/2013/RR-19), PCMCs PGI Yashwantrao Chavan Memorial Hospital (8th July 2022, ECR/1236/Inst/MH/2019) and Saideep Healthcare & Research Centre (19th July 2022, Reg. No. ECR/1644/Inst/MH/2022). The study was conducted in accordance with the Declaration of Helsinki, the International Conference for Harmonization guideline for Good Clinical Practice (GCP), and relevant health-related research guidelines of the Indian Ministry of Health and Family Welfare and the Indian Council of Medical Research. The study was prospectively registered in the Clinical Trial Registry of India (CTRI/2022/07/044154) and the results were reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
The study included six clinical visits: Visit 1 screening visit (day â7 to day 1), visit 2 randomisation/baseline (day 1), visit 3 follow-up (day 8 ± 1, week 1), visit 4 follow-up (day 15 ± 1, week 2), visit 5 follow-up (day 22 ± 1, week 3) and visit 6 follow-up (day 29 ± 1, week 4).
Study participants
Adults were eligible for inclusion if they were aged from 18 to 65 years, diagnosed with IBS-D (of any severity) as per ROME IV criteria (Drossman, 2016) with at least one Bristol Stool Form Scale (BSFS) type 6 or 7 stool on at least 2 days per week, with an average worst daily abdominal pain intensity (within the past 24 hours) of at least 3 points on a 0-10 point Numerical Rating Scale (NRS), and willing to participate in the study and provide informed consent. Exclusion criteria included constipation-predominant IBS, diarrhoea other than that associated with IBS and/or requiring antibiotic treatment, acute GI tract infection, other GI diseases, type 1 diabetes mellitus, uncontrolled type 2 diabetes mellitus, clinically significant and/or severe or unstable illnesses of the cardiovascular, pulmonary, neurological, psychiatric, endocrine, immune, respiratory, hepato-biliary, renal, urinary, haematological, musculoskeletal system and/or any inflammatory disorder, and known hypersensitivity to any of the ingredients in the study products that would preclude the safe administration of the study product; history of food allergies, lactose intolerance, celiac disease, inflammatory bowel disease, bowel cancer, bariatric surgery or surgical resection of the stomach, small intestine, or large intestine, unexplained weight loss, rectal bleeding, human immunodeficiency virus, hepatitis B, hepatitis C, or alcohol or drug abuse within three months prior to screening; use of antidepressant agents, unless used at a stable dose for at least two weeks prior to screening; intake of any probiotic, prebiotic or synbiotic formulations, antibiotics, bile acid sequestrants, serotonin type 3 receptor antagonists or medications for the treatment of IBS-D (e.g. eluxadoline) within two weeks prior to screening; females who were pregnant, lactating, or not willing to use contraceptives during the course of the study; and unwillingness or inability to comply with the study protocol and provide informed consent.
Participation in the study was voluntary and, prior to screening, written informed consent was obtained from all participants, after being fully informed about all study procedures and that they could withdraw from the study at any time.
Study intervention and blinding
Eligible participants were randomised into the test group (probiotic) or control group (placebo). The test group received a total daily dose of 4Â Ã 109 cfu B. subtilis HU58 and 2Â Ã 109 cfu H. faecalis SC208, to be taken in two divided doses with meals (2Â Ã 109 cfu B. subtilis HU58 and 1Â Ã 109 cfu H. faecalis SC208 per capsule) for 28 days. The control group received a placebo capsule which contained only the excipients present in the probiotic product (both manufactured and provided by Synergia Life Sciences [formerly known as Riata Life Sciences] Pvt Ltd, Vadodara, India) to be taken twice per day with a meal, for 28 days. Computer generated permuted block randomisation with a block size of four was used to randomise eligible participants into two groups with a 1:1 ratio. Group allocation was concealed from the participants, investigators and clinical staff by centralised preparation of probiotic and placebo capsules with a similar appearance, taste and smell, which were packed in identical high-density polyethylene bottles, labelled with a unique identification code according to the randomisation list, and dispensed sequentially by the blinded clinical staff. Group allocations remained concealed until the final database was locked.
Assessments and endpoints
The primary endpoint of the study was the percentage of overall responders for both abdominal pain and stool consistency at week 4 in each study group (USDHHS-FDA, 2012). A responder for abdominal pain was defined as a participant with a decrease in their weekly average abdominal pain NRS score of at least 30% from baseline to week 4. A responder for stool consistency was defined as a participant who experienced a decrease of at least 50% in the average number of days per week with at least one BSFS type 6 or 7 stool, from baseline to week 4. An overall responder was defined as a participant who met both these criteria, showing both a decrease of at least 30% in their weekly average abdominal pain NRS score and a decrease of at least 50% in the average number of days per week with at least one BSFS type 6 or 7 stool, from baseline to week 4. Clinical evaluation was performed during the study visits by the clinician. At baseline, participants were provided with a daily diary card to record study product intake, stool consistency (Bristol Stool Form Scale [BSFS], type 1-2 constipation; type 3-5 normal; type 6-7 loose stool or diarrhoea) (Lewis and Heaton, 1997) and abdominal pain intensity (worst abdominal pain within the last 24 hours) assessed using a 11-point Numerical Rating Scale [NRS] where 0 is no pain and 10 is the worst pain imaginable (McCaffery and Beebe, 1989), from which average weekly scores were calculated. During the study visits at week 1 to week 4, the investigator reviewed and verified the participantsâ diary cards and documented the number of days per week with at least one BSFS type 6 or 7 stool, and the occurrence of adverse events (AEs). Participant stress levels were assessed by the investigator at baseline and week 4 using the Perceived Stress Scale (PSS) (Cohen et al., 1983). Overall improvement in IBS symptoms was assessed by the investigator with the IBS Global Assessment of Improvement Scale (IBS-GAI) at week 4. Secondary study endpoints included the percentage of responders for stool consistency, the percentage of responders for abdominal pain, and the percentage of responders for IBS-GAI, defined as having either moderately or substantially improved symptoms (Passos et al., 2009), and the mean change from baseline in stool consistency (BSFS), abdominal pain intensity (NRS), and perceived stress (PSS) at weeks 1, 2, 3 and 4. Stool samples were collected at baseline and week 4, using the Zymo Feces catcher (Zymo Research Corp., Tustin, CA, USA) and placed in a sterile 50Â ml collection tube. Assessment of gut microbiota composition and total faecal SCFA levels were planned as exploratory endpoints. However, due to insufficient stool sample collection and quality, reliable analyses of the gut microbiome and SCFA levels could not be performed.
Safety assessment

CONSORT flow diagram of study.
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00113
Safety assessments included evaluation and grading of adverse events, monitoring of vital signs (temperature, pulse, systolic and diastolic blood pressure) and physical examination throughout the study period (visit 1 to visit 6).
Statistical analysis
Due to the exploratory nature of the study, the sample size was not based on a formal statistical power calculation. Statistical analysis was performed using SAS 9.1 (Cary, NC, USA) on the per protocol (PP) population, including all randomised participants who met all inclusion/exclusion criteria, consumed the study product every day, and completed the study up to week 4 without any major protocol deviation that might affect the results. Linear mixed models were fitted for the change from baseline in NRS score and stool consistency BSFS score, where treatment group, visit and the interaction between treatment group and visit were used as fixed terms, the corresponding baseline score as a covariate, and participant as the random term. The differences between the treatment groups over the visits and within each visit were estimated from the fitted models using least-square means (LSMs). In addition, within-group changes at each visit were calculated. The PSS score was analysed with analysis of covariance (ANCOVA) models, where the treatment group was used as the fixed term and the corresponding baseline value as a covariate. Chi-square and Fisherâs exact tests (for low (<5) cell counts) were used, respectively, for categorical data relating to gender, stool consistency (BSFS) categories and the proportion of responders. A P-value of <0.05 was considered statistically significant. Data are presented as mean (standard deviation) and proportion (n, %) of participants, unless otherwise stated.
3 Results
Participants
The number of participants who were included in each stage of the study is presented in a CONSORT flow diagram (Figure 1).
Participant characteristics
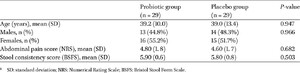
At baseline, there were no significant differences in participant characteristics between the two study groups (Table 1). Throughout the study, few concomitant medications were reported, of which most were vitamin and mineral supplements and paracetamol, and none related to the management of IBS-D, with no significant differences between groups.
Summary of participant characteristics at baseline.1
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00113
Response to probiotic
Overall responders for abdominal pain (NRS) and stool consistency (BSFS)
At week 4, there were significantly more overall responders for both abdominal pain and stool consistency in the probiotic group (n = 24, 82.8%) than the placebo group (n = 13, 44.8%) (
Abdominal pain (NRS)
At baseline, there were no statistically significant differences in mean NRS scores for abdominal pain intensity between groups (Table 1). NRS scores significantly decreased at all timepoints within each group (
Change from baseline in abdominal pain intensity assessed by Numerical Rating Scale (NRS) at each timepoint in the probiotic versus placebo group. Values are presented as mean and standard error of mean (SEM) error bars *
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00113
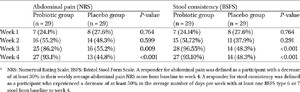
The proportion of responders for abdominal pain in each group are presented in Table 2. Throughout the study, the proportion of responders for abdominal pain increased at each timepoint in the probiotic group, with the majority of participants in this group being responders at week 4. Conversely, in the placebo group, the proportion of responders increased slightly from week 1 to week 3, followed by a reduction to less than half of participants by week 4. Consequently, whilst there were no significant differences between groups at week 1 or 2, there were significantly more responders for abdominal pain in the probiotic group compared to the placebo group at week 3 (86.2% versus 55.2%,
Proportion of participants (n [%]) who were responders for abdominal pain and stool consistency, respectively1
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00113
Stool consistency (BSFS)
At baseline, there were no significant differences in mean BSFS scores between groups (Table 1). During the study, there were statistically significant decreases in BSFS scores at all timepoints within each group (
Change from baseline in stool consistency assessed by Bristol Stool Form Scale (BSFS) at each timepoint in the probiotic versus placebo group. Values are presented as mean and standard error of mean (SEM) error bars. *
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00113
Whilst the proportion of responders for stool consistency increased throughout the study in both groups, there were significantly more responders within the probiotic group compared to the placebo group by week 3 (96.6% versus 48.3%,
IBS global improvement (IBS-GAI)
At week 4, there were significantly more responders for the IBS-GAI scale in the probiotic group compared to the placebo group (72.4% versus 41.4%,
Perceived stress scale (PSS)
At baseline, mean PSS scores were similar, with no significant differences between the probiotic and placebo groups (19.7 [SD 4.08] versus 21.0 [SD 3.95],
Gut microbiota diversity and faecal short-chain fatty acid (SCFA) levels
Gut microbiota and faecal SCFA analysis could not be completed due to an insufficient number of analysable stool samples (56 samples from 29 participants), precluding reliable statistical interpretation.
Safety (adverse events, AEs)
During the study, two AEs (fever and constipation) were recorded in one participant from the placebo group. Both were categorised as mild severity and unlikely to be related to the use of study product.
4 Discussion
This randomised, double-blind, placebo-controlled pilot trial was the first to demonstrate that 4 weeks of supplementation with the dual-strain combination of B. subtilis (HU58) and H. faecalis (SC208) led to significant improvements in abdominal pain, diarrhoea, and global symptoms of IBS-D in adults, adding to the growing evidence base for the safety and efficacy of this spore-forming probiotic combination in individuals with diarrhoea, compared to placebo.
Placebo responses are well documented in IBS trials, particularly for subjective outcomes such as abdominal pain and global symptom scores, but have also been observed for bowel habitârelated endpoints, including stool frequency and consistency. In disorders of gutâbrain interaction (DGBI), placebo effects may extend beyond symptom perception and involve physiological modulation of gastrointestinal motility and secretion through gutâbrain axis pathways influenced by expectancy and stress-related mechanisms (Drossman, 2016; Enck et al., 2013; Enck and Klosterhalfen, 2005). Despite this, in the present study the improvements observed in the probiotic group were greater than those in the placebo group, supporting a specific beneficial effect of B. subtilis HU58 and H. faecalis SC208 on GI symptoms.
Previous studies have shown similar positive effects of this probiotic combination on the duration and severity of diarrhoea and the intensity of associated abdominal pain, in adult and paediatric populations with AAD and acute infective diarrhoea, respectively (Dhongade, 2022, Mehta, 2020a). Whilst the present study demonstrated benefits by week 3, resolution of acute diarrheal symptoms was reported within seven days of the administration of B. subtilis HU58 and H. faecalis SC208 in the previous studies, reflecting perhaps a greater baseline symptom severity and potentially different mechanisms by which these strains may have exerted positive effects on the respective study cohorts, each with a different aetiology of diarrheal symptoms. For example, in an antibiotic-induced dysbiosis in vitro inflammatory bowel disease model, B. subtilis HU58 and H. faecalis SC208 were shown to increase gut barrier integrity and reduce proinflammatory cytokines including tumour-necrosis factor-α, monocyte chemoattractant protein-1 and interleukin-6 levels within two weeks (Marzorati et al., 2020), whilst their specific mode of action in IBS-D has not yet been clarified. Furthermore, studies of other probiotic strains conducted in IBS-D populations have reported improved symptoms around four to eight weeks after the administration of probiotics, which is later than the three weeks of the present study, and which may indicate the typical timeframe required for probiotic effects to be seen in this population (Dolin, 2009; Majeed et al., 2016; Sun et al., 2018).
In contrast to the improvements in GI symptoms, whilst there was a statistically significant decrease in perceived stress levels in the probiotic group, this was also observed in the placebo group, resulting in a non-significant difference between groups in the present study. Previous trials have demonstrated strong placebo effects on stress-related outcomes, possibly due to the routine of preparing and taking the intervention and the associated hope of improvement having a positive effect on mood (Merkouris et al., 2024). Nevertheless, as a DGBI (Drossman, 2016), the association between stress and IBS is well documented with concurrent improvements in stress levels and IBS symptoms having been observed (Horn et al., 2023). In particular, probiotics may exert positive effects on GI symptoms in part through the mediation of the gut-brain axis through SCFA production, which in turn influences the release of serotonin and other neurotransmitters known to contribute to the regulation of mood and stress response pathways (Cheng et al., 2022, Silva et al., 2020). Unfortunately, in the present study it was not possible to assess whether the improvements in diarrhoea, abdominal pain and global symptoms were accompanied by changes in SCFA production, due to insufficient analysable stool samples. In fact, studies have shown contradictory findings relating to SCFA levels in IBS-D populations, with some reporting higher faecal concentrations of acetate, propionate, and total SCFA compared to healthy individuals, related perhaps to an increased colonic fermentation in IBS-D (Sun et al., 2019). Future research should involve a larger cohort, placebo lead-in period, and longer intervention period to support the detection of changes in perceived stress and total and specific SCFA concentrations, such as propionate and butyrate following probiotic supplementation, and to enable exploration of possible correlations between these endpoints and the gut microbiota.
Indeed, an additional exploratory endpoint of the present study was the effect of the B. subtilis HU58 and H. faecalis SC208 spores on gut biodiversity, which was precluded by the insufficient samples amenable to statistical analysis. To date, relatively few studies investigating probiotic supplementation in IBS-D populations have explored changes to intestinal microbiota, possibly due to the logistical challenges associated with collecting and sequencing commensurate samples. In one study, synbiotic supplementation over a four-month period was not associated with increases in alpha diversity, but did increase the relative abundance of the supplemented probiotic species including B. coagulans (Phan et al., 2021). By contrast, studies which have investigated the effects of probiotics on the gut microbiota over four to eight weeks have failed to demonstrate significant changes, perhaps indicating the strain-specific nature of probiotic interactions with the commensal gut microbes, and the need for a longer intervention period than that found in the present study (Ng et al., 2023). In general, probiotic supplementation is thought to exert only transient changes to the gut microbiota composition over the duration of intake, with few microbes demonstrating the ability to permanently colonise the GI tract (Zmora et al., 2018).The present study had some limitations that should be considered for future research. As a pilot study, the small study population, short intervention period and lack of placebo lead-in were insufficient to power a reliable statistical analysis of the effects of these probiotic spores on the secondary and exploratory endpoints relating to perceived stress, gut microbiota and SCFA levels. It was not possible to report on gut microbiota and SCFA changes as initially planned, due to inadequate sample collection and sequencing, which precluded investigation of whether B. subtilis HU58 and H. faecalis SC208 may modulate or colonise the intestinal ecosystem and exploration of their potential mechanisms of action. In general, analysis of the per protocol population may overestimate the probiotic effect size compared to intention to treat (ITT) analysis. However, as there were no major protocol deviations detected during the study and only three early drop-outs (4.9% of the total cohort) were excluded from the per protocol population, the intention to treat analyses would have yielded identical results to the per protocol population for the primary endpoint at week 4, and were therefore omitted. Notwithstanding these limitations, potential confounding variables were controlled for with use of randomisation, placebo, blinding of participants and research personnel, and inclusion of baseline NRS and stool BSFS scores as covariates in the statistical methods, which increased the reliability of the results.
Overall, the findings of this randomised, double-blind, placebo-controlled pilot study provide evidence to suggest that the combination of B. subtilis HU58 and H. faecalis SC208 is effective in improving GI symptoms in an IBS-D population. Collectively the body of evidence from this and previously published studies of B. subtilis HU58 and H. faecalis SC208 (Dhongade, 2022, Mehta, 2020a) may support the effectiveness of these spore-forming probiotic strains on diarrheal symptoms in general, irrespective of aetiology. It is possible that similar positive outcomes may be seen in individuals with symptoms of diarrhoea from other causes, and further research investigating the effects of these strains among a broader study population is warranted to confirm this. While some beneficial effects may reflect general properties of Bacillus spore-formers, the observed improvements in this study may also be strain-specific, highlighting the need for future mechanistic studies to determine whether B. subtilis HU58 and H. faecalis SC208 exert unique effects compared to other spore-forming strains.
5 Conclusions
The findings of this randomised, double-blind, placebo-controlled pilot study suggest that the combination of B. subtilis HU58 and H. faecalis SC208 is safe and effective in improving stool consistency and abdominal pain in individuals with IBS-D. The consistency of these findings with those of previous clinical trials of individuals with AAD and acute infective diarrhoea may indicate a broad applicability of these strains in the management of diarrheal symptoms. Further clinical studies with a larger study population, longer intervention period and robust faecal microbiota and SCFA sampling, sequencing techniques and metabolomic analysis are required to better understand the effect of these spore-forming bacterial strains on the gut microbial community and the potential mechanisms by which they exert positive effects.
Corresponding author; e-mail:Â kass@novonesis.com
Acknowledgements
This research was sponsored and funded by Synergia Life Sciences Pvt. Ltd., since acquired by Novozymes A/S (part of the Novonesis group). The authors would like to thank Biosphere Clinical Research (Maharashtra, India) who supported this study.
Authorsâ contribution
Conceptualization: SJ; Data curation: SJ; Formal analysis: SJ; Investigation: SK, AP, BLD, PS, DS; Methodology: SJ; Project administration: SJ; Resources: SJ; Supervision: SJ; Validation: KS, CH, SJ; Visualization: KS, CH, SJ; Writing â original draft: KS; Writing â review & editing: KS, CH, SJ. All authors have read and agreed to the published version of the manuscript.
Conflict of interest
This study was sponsored and fully funded by Synergia Life Sciences Pvt. Ltd., since acquired by Novozymes A/S (part of the Novonesis group), who manufacture the probiotic strains Bacillus subtilis (HU58â¢) and Heyndrickxia faecalis (SC208â¢). HU58 and SC208 are registered trademarks by Synergia Life Sciences Pvt. Ltd. Katy Sorensen, Caterina Holz and Shashank Jadhav are employed by entities of the Novonesis group. Sanjeev Khanna, Ashwin Porwal, BL Dharmendra, Pravin Soni and Deepak Siddavaram have no financial or non-financial interests to declare.
References
Casula, G. and Cutting, S.M., 2002. Bacillus probiotics: spore germination in the gastrointestinal tract. Applied and Environmental Microbiology 68(5): 2344-2352. https://doi.org/10.1128/aem.68.5.2344-2352.2002
Cheng, Y., Liu, J. and Ling, Z., 2022. Short-chain fatty acids-producing probiotics: A novel source of psychobiotics. Critical Reviews in Food Science and Nutrition 62(28): 7929-7959. https://doi.org/10.1080/10408398.2021.1920884
Cohen, S., Kamarck, T. and Mermelstein, R., 1983. A global measure of perceived stress. Journal of Health and Social Behavior 24(4): 385-396. https://doi.org/10.2307/2136404
Cutting, S.M., 2011. Bacillus probiotics. Food Microbiology 28(2): 214-220. https://doi.org/10.1016/j.fm.2010.03.007
Dawoodi, S., Dawoodi, I. and Dixit, P., 2022. Gastrointestinal problem among Indian adults: Evidence from longitudinal aging study in India 2017-18. Frontiers in Public Health 10: 911354. https://doi.org/10.3389/fpubh.2022.911354
De Castro Soares, G.G., Marinho, C.H., Pitol, R., Andretta, C., Oliveira, E., Martins, C. and Riella, M.C., 2017. Sporulated Bacillus as alternative treatment for diarrhea of hospitalized adult patients under enteral nutrition: A pilot randomized controlled study. Clinical Nutrition ESPEN 22: 13-18. https://doi.org/10.1016/j.clnesp.2017.08.006
Dhongade, A.J., Kulkarni, S., Jadhav, S., Nargundkar, N., Deshmukh, D. and Mehta, A., 2022. The efficacy and safety of a Bacillus probiotic combination for the treatment of acute diarrhea in children: a double-blind, randomized, placebo-controlled multicentric study. Pediatric Infectious Disease Journal 4: 86-91. https://doi.org/10.5005/jp-journals-10081-1370
Dolin, B.J., 2009. Effects of a proprietary Bacillus coagulans preparation on symptoms of diarrhea-predominant irritable bowel syndrome. Methods and Findings in Experimental and Clinical Pharmacology 31(10): 655-659. https://doi.org/10.1358/mf.2009.31.10.1441078
Dound, Y.A., Jadhav, S.S., Devale, M., Bayne, T., Krishnan, K. and Mehta, D.S., 2017. The effect of probiotic Bacillus subtilis HU58 on immune function in healthy human. The Indian Practitioner 70(9): 15-20.
Drossman, D.A., 2016. Functional gastrointestinal disorders: history, pathophysiology, clinical features, and Rome IV. Gastroenterology 150(6): 1262-1279.e2. https://doi.org/10.1053/j.gastro.2016.02.032
Enck, P. and Klosterhalfen, S., 2005. The placebo response in functional bowel disorders: perspectives and putative mechanisms. Journal of Neurogastroenterology and Motility 17(3): 325-331. https://doi.org/10.1111/j.1365-2982.2005.00676.x
Enck, P., Bingel, U., Schedlowski, M. and Rief, W., 2013. The placebo response in medicine: minimize, maximize or personalize? Nature Reviews Drug Discovery 12(3): 191-204. https://doi.org/10.1038/nrd3923
Food Safety and Standards Authority of India (FSSAI), 2022. Direction under Section 16(5) of the Food Safety and Standards Act, 2006 regarding operationalization of FSS (Health Supplements, Nutraceuticals, Food for Special Dietary Use, Food for Special Medical Purpose and Prebiotic and Probiotic Food) Regulations, 2022 [FSS (Nutra) Regulations, 2022]. New Delhi: FSSAI, 29 March 2022.
Fusco, W., Lorenzo, M.B., Cintoni, M., Porcari, S., Rinninella, E., Kaitsas, F., Lener, E., Mele, M.C., Gasbarrini, A., Collado, M.C., Cammarota, G. and Ianiro, G., 2023. Short-chain fatty-acid-producing bacteria: key components of the human gut microbiota. Nutrients 15(9): 2211 https://doi.org/10.3390/nu15092211
Guarner, F., Sanders, M., Szajewska, H., Cohen, H., Eliakim, R., Herrera, C., Karakan, T., Merenstein, D., Piscoya, A., Ramakrishna, B. and Salminen, S., 2023. World Gastroenterology Organisation Global Guidelines â Probiotics and prebiotics. World Gastroenterology Organisation. Available at: https://www.worldgastroenterology.org/UserFiles/file/guidelines/probiotics-and-prebiotics-english-2023.pdf
Hong, H.A., Duc le, H. and Cutting, S.M., 2005. The use of bacterial spore formers as probiotics. FEMS Microbiology Reviews 29(4): 813-835. https://doi.org/10.1016/j.femsre.2004.12.001
Hong, H.A., Khaneja, R., Tam, N.M., Cazzato, A., Tan, S., Urdaci, M., Brisson, A., Gasbarrini, A., Barnes, I. and Cutting, S.M., 2009a. Bacillus subtilis isolated from the human gastrointestinal tract. Research in Microbiology 160(2): 134-143. https://doi.org/10.1016/j.resmic.2008.11.002
Hong, H.A., To, E., Fakhry, S., Baccigalupi, L., Ricca, E. and Cutting, S.M., 2009b. Defining the natural habitat of Bacillus spore-formers. Research in Microbiology 160(6): 375-379. https://doi.org/10.1016/j.resmic.2009.06.006
Horn, A., Stangl, S., Parisi, S., Bauer, N., Roll, J., Löffler, C., GaÌgyor, I., Haas, K., Heuschmann, P.U., Langhorst, J. and Keil, T., 2023. Systematic review with meta-analysis: Stress-management interventions for patients with irritable bowel syndrome. Stress and Health 39(4): 694-707. https://doi.org/10.1002/smi.3226
Lewis, S.J. and Heaton, K.W., 1997. Stool form scale as a useful guide to intestinal transit time. Scandinavian Journal of Gastroenterology 32(9): 920-924. https://doi.org/10.3109/00365529709011203.
Majeed, M., Nagabhushanam, K., Natarajan, S., Sivakumar, A., Ali, F., Pande, A., Majeed, S. and Karri, S.K., 2016. Bacillus coagulans MTCC 5856 supplementation in the management of diarrhea predominant Irritable Bowel Syndrome: a double blind randomized placebo controlled pilot clinical study. Nutrition Journal 15: 21. https://doi.org/10.1186/s12937-016-0140-6
Marzorati, M., Abbeele, P.V.D., Bubeck, S.S., Bayne, T., Krishnan, K., Young, A., Mehta, D. and DeSouza, A., 2020. Bacillus subtilis HU58 and Bacillus coagulans SC208 Probiotics reduced the effects of antibiotic-induced gut microbiome dysbiosis in an M-SHIME((R)) model. Microorganisms 8(7): 1028. https://doi.org/10.3390/microorganisms8071028
McCaffery, M. and Beebe, A., 1989. Pain: Clinical Manual for Nursing Practice. C.V. Mosby Company, St. Louis, USA.
Mehta, D.S., de Souza, A., Jadhav, S. and Devale, M., 2020a. An open labeled, placebo controlled trial to evaluate the role of probiotics â Bacillus subtilis HU58 and Bacillus coagulans SC208 on antibiotic associated diarrhea in humans. Biomedical Journal of Scientific & Technical Research 29(4): 22679-22684. https://doi.org/10.26717/BJSTR.2020.29.004839
Mehta, D.S., de Souza, A., Jadhav, S. and Devale, M., 2020b. A study of probiotic Bacillus subtilis HU58 for the management of antibiotic-associated diarrhoea in adults. Indian Practitioner 73(4): 22-28.
Merkouris, E., Mavroudi, T., Miliotas, D., Tsiptsios, D., Serdari, A., Christidi, F., Doskas, T.K., Mueller, C. and Tsamakis, K., 2024. Probioticsâ effects in the treatment of anxiety and depression: a comprehensive review of 2014-2023 clinical trials. Microorganisms 12(2): 411. https://doi.org/10.3390/microorganisms12020411
Narsing Rao, M.P., Banerjee, A., Liu, G.-H. and Thamchaipenet, A., 2023. Genome-based reclassification of Bacillus acidicola, Bacillus pervagus and the genera Heyndrickxia, Margalitia and Weizmannia. International Journal of Systematic and Evolutionary Microbiology 73(7): 5961. https://doi.org/10.1099/ijsem.0.005961
Ng, Q.X., Lim, Y.L., Yaow, C.Y.L., Ng, W.K., Thumboo, J. and Liew, T.M., 2023. Effect of probiotic supplementation on gut microbiota in patients with major depressive disorders: a systematic review. Nutrients 15(6): 1351. https://doi.org/10.3390/nu15061351
Oka, P., Parr, H., Barberio, B., Black, C.J., Savarino, E.V. and Ford, A.C., 2020. Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: a systematic review and meta-analysis. The Lancet Gastroenterology & Hepatology 5(10): 908-917. https://doi.org/10.1016/s2468-1253(20)30217-x
Passos, M.C., Lembo, A.J., Conboy, L.A., Kaptchuk, T.J., Kelly, J.M., Quilty, M.T., Kerr, C.E., Jacobson, E.E., Hu, R., Friedlander, E. and Drossman, D.A., 2009. Adequate relief in a treatment trial with IBS patients: a prospective assessment. American Journal of Gastroenterology 104(4): 912-919. https://doi.org/10.1038/ajg.2009.13
Permpoonpattana, P., Hong, H.A., Khaneja, R. and Cutting, S.M., 2012. Evaluation of Bacillus subtilis strains as probiotics and their potential as a food ingredient. Beneficial Microbes 3(2): 127-135. https://doi.org/10.3920/Bm2012.0002
Phan, J., Nair, D., Jain, S., Montagne, T., Flores, D.V., Nguyen, A., Dietsche, S., Gombar, S. and Cotter, P., 2021. Alterations in gut microbiome composition and function in irritable bowel syndrome and increased probiotic abundance with daily supplementation. mSystems 6(6): e0121521. https://doi.org/10.1128/mSystems.01215-21
Silva, Y.P., Bernardi, A. and Frozza, R.L., 2020. The role of short-chain fatty acids from gut microbiota in gut-brain communication. Frontiers in Endocrinology 11: 25. https://doi.org/10.3389/fendo.2020.00025
Singh, P., Staller, K., Barshop, K., Dai, E., Newman, J., Yoon, S., Castel, S. and Kuo, B., 2015. Patients with irritable bowel syndrome-diarrhea have lower disease-specific quality of life than irritable bowel syndrome-constipation. World Journal of Gastroenterology 21(26): 8103-8109. https://doi.org/10.3748/wjg.v21.i26.8103
Sperber, A.D., Bangdiwala, S.I., Drossman, D.A., Ghoshal, U.C., Simren, M., Tack, J., Whitehead, W.E., Dumitrascu, D.L., Fang, X., Fukudo, S., Kellow, J., Okeke, E., Quigley, E.M.M., Schmulson, M., Whorwell, P., Archampong, T., Adibi, P., Andresen, V., Benninga, M.A., Bonaz, B., Bor, S., Fernandez, L.B., Choi, S.C., Corazziari, E.S., Francisconi, C., Hani, A., Lazebnik, L., Lee, Y.Y., Mulak, A., Rahman, M.M., Santos, J., Setshedi, M., Syam, A.F., Vanner, S., Wong, R.K., Lopez-Colombo, A., Costa, V., Dickman, R., Kanazawa, M., Keshteli, A.H., Khatun, R., Maleki, I., Poitras, P., Pratap, N., Stefanyuk, O., Thomson, S., Zeevenhooven, J. and Palsson, O.S., 2021. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome foundation global study. Gastroenterology 160(1): 99-114.e3. https://doi.org/10.1053/j.gastro.2020.04.014
Sun, Q., Jia, Q., Song, L. and Duan, L., 2019. Alterations in fecal short-chain fatty acids in patients with irritable bowel syndrome: A systematic review and meta-analysis. Medicine 98(7): e14513. https://doi.org/10.1097/md.0000000000014513
Sun, Y., Li, M., Li, Y.Y., Li, L.X., Zhai, W.Z., Wang, P., Yang, X.X., Gu, X., Song, L.J., Li, Z., Zuo, X.L. and Li, Y.Q., 2018. The effect of Clostridium butyricum on symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. Scientific Reports 8(1): 2964. https://doi.org/10.1038/s41598-018-21241-z
Tielemans, M.M., Jaspers Focks, J., van Rossum, L.G., Eikendal, T., Jansen, J.B., Laheij, R.J. and Van Oijen, M.G., 2013. Gastrointestinal symptoms are still prevalent and negatively impact health-related quality of life: a large cross-sectional population based study in the Netherlands. PLoS ONE 8(7): e69876. https://doi.org/10.1371/journal.pone.0069876
United States Department of Health and Human Services â Food and Drug Administration (USDHHS-FDA), 2012. Guidance for Industry. Irritable bowel syndrome â Clinical Evaluation of Drugs for Treatment. USDHHS-FDA Center for Drug Evaluation and Research. Available at: www.fda.gov/downloads/Drugs/Guidances/UCM205269.pdf.
Valdes, A.M., Walter, J., Segal, E. and Spector, T.D., 2018. Role of the gut microbiota in nutrition and health. British Medical Journal 361: k2179. https://doi.org/10.1136/bmj.k2179
Wei, L., Singh, R., Ro, S. and Ghoshal, U.C., 2021. Gut microbiota dysbiosis in functional gastrointestinal disorders: Underpinning the symptoms and pathophysiology. JGH Open 5(9): 976-987. https://doi.org/10.1002/jgh3.12528
Zmora, N., Zilberman-Schapira, G., Suez, J., Mor, U., Dori-Bachash, M., Bashiardes, S., Kotler, E., Zur, M., Regev-Lehavi, D., Brik, R.B., Federici, S., Cohen, Y., Linevsky, R., Rothschild, D., Moor, A.E., Ben-Moshe, S., Harmelin, A., Itzkovitz, S., Maharshak, N., Shibolet, O., Shapiro, H., Pevsner-Fischer, M., Sharon, I., Halpern, Z., Segal, E. and Elinav, E., 2018. Personalized gut mucosal colonization resistance to empiric probiotics is associated with unique host and microbiome features. Cell 174(6): 1388-1405.e21. https://doi.org/10.1016/j.cell.2018.08.041




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}