Abstract
Several studies have documented the safety and tolerance of probiotics in infants, however, most studies have been conducted with supplements. This randomised, double-blind, multicenter trial evaluated growth of healthy term infants fed infant formula supplemented with Limosilactobacillus reuteri DSM17938 (L. reuteri;
1 Introduction
A greater understanding of human milk composition and the differences between breastfed and formula-fed infants have provided opportunities to continuously improve formulas for infants unable to be breastfed. One major difference between breastfed and formula-fed infants is a difference in gut microbiota composition, which may result in a lower incidence of infections and morbidity in breastfed infants (Odiase et al., 2023; Stuebe, 2009).
In breastfed full-term infants, lactobacilli and bifidobacteria begin to appear in the stool by the third day of life (Yao et al., 2021). Bifidobacterium then becomes the dominant organism, representing 80% to 90% of the gut ecosystem. Formula-fed infants are colonised by a more diverse microbiota (Yang et al., 2016), These differences in the composition of the intestinal microbiota appear to be related to the more acidic environment of the gut in breastfed children (Duar et al., 2020), which tends to favour the predominance of bifidobacteria and inhibit the growth of potentially pathogenic bacteria (Gibson and Roberfroid, 1995).
Adding probiotics to infant formulas is intended to improve the intestinal microbiota of formula-fed infants. The addition of specific probiotics (e.g. strains of bifidobacteria) may also help improve the growth of infants, particularly in vulnerable populations (Steenhout et al., 2009). Several probiotics have been evaluated in randomised, controlled, double-blind clinical trials of infants and toddlers and have been shown to be safe and well-tolerated (Chouraqui et al., 2008; Gibson et al., 2009; Radke et al., 2017; Shen et al., 2024; Steenhout et al., 2009; Weizman et al., 2005). Probiotics such as Bifidobacterium animalis subspecies lactis (B. lactis) CNCM I-3446 have been shown to reduce the incidence of diarrhoea (Chouraqui et al., 2004; Saavedra et al., 1994), diaper rash (Hertiš Petek et al., 2022; Saavedra et al., 1998), and hard stools (Saavedra et al., 1998) in a number of infant and toddler trials, while oral administration of Limosilactobacillus reuteri (L. reuteri) DSM 17938, has been reported to reduce colic (Savino et al., 2007), improve gastric emptying (Indrio et al., 2008; 2011), and reduce regurgitation (Indrio et al., 2008; 2011) in infants. Two other probiotics commonly added to infant formulas include Bifidobacterium longum ATCC BAA-999 and Lacticaseibacillus rhamnosus CGMCC 1.3724. Both have been shown to be safe and well tolerated as supplements in infant formulas (Berseth et al., 2024; Hascoet et al., 2011; Shulman et al., 2022). In older infants, above six months of age, the combination of L. rhamnosus and B. longum in a follow-on-formula matrix has been tested in only one previous study conducted in France (Chouraqui et al., 2008), showing the combination to be safe and well tolerated. However, evidence from different geographies is lacking.
Although the safety of infant formulas containing probiotics has been demonstrated in a variety of infant populations (Gibson et al., 2009; Papagaroufalis et al., 2014; Soh et al., 2009; Underwood et al., 2013; Weizman et al., 2005), safety and tolerance data in Indian infants are lacking. Evaluating the safety of infant formula with regard to growth is particularly important in India, a region in which growth failure remains a persistent challenge (Lundeen et al., 2014; Saji et al., 2024). Consequently, the primary objective of the present study was to evaluate weight gain in infants in India who received one of two infant formulas supplemented with probiotics, either L. reuteri or B. lactis, or the same infant formula without probiotics through 6 months of age. Secondary objectives included the assessment of the impact of these probiotic-supplemented formulas on GI tolerance, adverse events (AEs), as well as fecal microbiota and urinary D-lactate until 12 months of age.
2 Materials and methods
Study design
This was a prospective, multicenter, randomised, double-blind study to evaluate the safety and tolerance of infant formulas containing probiotics Limosilactobacillus reuteri (L. reuteri DSM17938) or Bifidobacterium lactis (B. lactis CNCM I-3446) in healthy term infants in India. The study was conducted between August 2010 and July 2012 at five centres in India (CTRI/2010/091/001111 (Clinical Trials Registry – India; www.ctri.nic.in)). The study protocol and informed consent form were reviewed and approved by an Independent Ethics Committee at each centre. Written informed consent was obtained from the infants’ parents or legal guardian prior to enrolment.
Population
The study population consisted of healthy, full-term infants ≥2 weeks to 3 months of age at enrolment who required mixed feeding (i.e. breast milk and formula in any proportion) due to partial lactation failure or informed choice by the mother. Eligible infants had a gestational age of 37-42 weeks and a birth weight of 2,500-4,500 g. Exclusion criteria included infants from an HIV-positive mother or mother with gestational diabetes; any significant illness or malformation that could affect normal growth; and re-hospitalisation prior to enrolment for more than two days (except those re-hospitalised due to jaundice). Infants were openly allocated to either exclusive breastfeeding or mixed feeding groups. Within the mixed-fed group, blinded random allocation, stratified by sex and centre, was conducted to assign infants to one of the three study formulas (randomisation lists were produced using R version 2.6.1).
Study formulas
Mixed-fed infants were randomised in a 1:1:1 ratio to one of three feeding groups: mixed feeding with infant formula containing the probiotic L. reuteri DSM17938 (2 × 107 cfu/g of powder, equivalent to a daily intake of 2.4 × 109 cfu; the L. reuteri group); mixed feeding with infant formula containing the probiotic B. lactis CNCM I-3446 (1.8 × 107 cfu/g of powder, equivalent to a daily intake of 2.2 × 109 cfu; the B. lactis group); or mixed feeding with a standard control formula not containing probiotics (the standard group). Each infant formula contained adequate amounts of energy (670 kcal/l), protein (2.4 g/100 kcal, casein:whey ratio of 60:40), and other nutrients to support the normal growth of healthy infants. Parents/caregivers were instructed to follow guidelines printed on the label regarding appropriate volumes of formula to be offered per day. Breastfed infants received exclusive breast milk until the end of the 6th month of age. For infants stopping breastfeeding during the 5th and 6th month of age, an infant formula without probiotics was provided until the end of 6 months. No other food was given to infants during the first 6 months of life. However, complementary foods other than the study formulas were permitted to be introduced gradually after age 6 months.
When these enrolled mixed-fed infants reached 7 months of age, they received the following assigned follow-up formulas until age 12 months: the L. reuteri group received follow-up formula supplemented with L. reuteri (1.9 × 107 cfu/g of powder, equivalent to a daily intake of 2.1 × 109 cfu). To address the gap in the literature on the safety and tolerability of the combined use of L. rhamnosus and B. longum; the B. lactis group received follow-up formula supplemented with L. rhamnosus (CGMCC 1.3724) hereafter L. rhamnosus LPR (1.5 × 107 cfu/g of powder, equivalent to a daily intake of 1.7 × 109 cfu) and B. longum ATCC BAA-999 (7.8 × 106 cfu/g of powder, equivalent to a daily intake of 8.8 × 108 cfu) hereafter B. longum BL999 and the standard group received follow-up formula without probiotics. Breastfed infants continued to receive exclusive breast milk or mixed feeding with follow-up formula with probiotics L. rhamnosus LPR and B. longum BL999, according to the parent’s choice.
The investigators, study staff, and parents were blinded to the identities of the formulas.
Observation period
Infant demographic and anthropometric data were collected from birth records and at the enrolment visit. Enrolment was conducted between 2 weeks and 3 months after birth. Clinic visits were scheduled at 1.5, 2, 2.5, 3.5, 4.5, 6, 8, 10, and 12 months (visits 1-9) to dispense formula, collect anthropometry data, and record AEs (since the enrolment age could vary, the first three visits did not apply to some subjects). Parents were asked to record the feeding history of their infants for 3 consecutive days prior to each visit, up until 6 months only. Feeding history included volume of formula consumed and the number of formula feedings or number of breastfeeds per day. The volume of breast milk provided was not collected at any time. Parents/caregivers also recorded gastrointestinal (GI) tolerance for 3 consecutive days immediately prior to each of the clinic visits until 6 months in an at home diary.
Outcomes
Growth and other anthropometric measurements
The primary outcome for this study was weight gain (g/day) from baseline (visit 0) to 6 months of age (visit 6). The primary hypothesis of the study was that the mean weight gain of infants fed an infant formula containing either L. reuteri or B. lactis up to 6 months of age is not inferior to the growth observed in infants fed with an infant formula without probiotics.
Infant weight was assessed at each clinic visit and rounded to the nearest 10 g. Infants were weighed without clothing or nappy/diaper on calibrated electronic weighing scales, with the same scales used for all infants at all visits.
Other anthropometric parameters assessed from birth to 12 months included length, body mass index (BMI), head circumference gains, and corresponding WHO z-scores. Recumbent length was measured at each visit in centimetres (±1 mm) using a standardised length board. Head circumference (±1 mm) was measured approx. 2.5 cm above the eyebrows, directly over the largest circumference of the skull.
Digestive tolerance
Digestive tolerance was determined by the investigator at each visit up to 6 months of age based on parents’ reports of stool consistency and frequency (number of stools per 24 h), spitting up (no/sometimes/often), vomiting (no/sometimes/often), flatulence (no/sometimes/often), irritability/fussiness (yes/no, and if so for how many hours), and sleeping habits (number of times waking during the night, longest period of uninterrupted sleep). All information on the child’s stooling pattern and other GI tolerance symptoms was recorded in diaries by parents/caregivers for the 3 consecutive days immediately prior to each of the clinic visits until age 6 months. The investigator confirmed the child’s digestive tolerance based on a review of these diaries at each study visit.
Adverse events
Adverse events were collected at each visit throughout the entire 12-month study period, with a focus on diarrhoea and upper respiratory tract infections (including bronchiolitis and otitis media). Any episodes of illness occurring since the last visit were recorded as AEs. Conditions associated with morbidity were predefined by investigators to help caregivers assess these events, including diarrhoea (defined as 3 or more loose or watery stools per day, with an episode of diarrhoea considered to have ended once there have been 2 consecutive non-watery stools, or no stools for 24 h); respiratory symptoms (defined as runny nose or chronic cough recorded on a scale from 0 to 3 (0: absent; 1: mild; 2: moderate; 3: severe); fever (defined as when the infant’s temperature was above 38 °C, reaching 38.5 °C at least once during the last 24 h); eczema (recorded on a scale from 0 to 3, similar to the one described for respiratory symptoms) and constipation (defined as when the infant does not pass a stool for ≥3 consecutive days, with stools that are hard, dry, and painful to pass).
Abundance of key bacteria in fecal matter
At 4.5 months of age, a stool sample was obtained at home by the parents/caregivers in a subset of approximately 30 subjects per group in appropriate conditions, defined as less than 15 h between stool emission and stool processing at the laboratory. Lactobacillus, Bifidobacterium, Clostridium perfringens, Enterobacteriaceae, Bacteroides/Prevotella, and total bacteria populations were analysed by fluorescent in situ hybridisation (BioVisible, Groningen, The Netherlands). B. lactis and L. reuteri detection was performed by an external laboratory (Advanced Analytical Technologies, Piacenza, Italy) following the AAT internal protocol for L. reuteri and B. lactis detection that consisted in plating of the samples on Bifidobacterium spp. selective medium, counting CFU before scraping of plates surface and recovery of grown colonies, cells disruption of the plates triplicate by means of Maxwell protocol AAT procedure. This later allowed identification of the presence of the probiotic B. lactis by strain-specific polymerase chain reaction (detection limit 103 CFU/g feces). Specific primers used for B. lactis were (sequence 5′ → 3′): sense GAGCTGATCGACGACCTGAC and anti-sense CCGAGAAAATCTGGGATGAG8 (Baglatzi et al., 2016).
Urinary d-lactate
Following 2 months of formula- or breast-feeding, urinary samples were collected in a subset of approximately 15 subjects per group to analyse creatinine, d-lactate, l-lactate, % of d-lactate/l-lactate, and sum of d-lactate and l-lactate. Infants were included in this group if their parents or caregivers were willing and able to provide urine samples on their behalf. Samples were collected by study staff using a sterile urine collection bag approximately 2 h after the last feed. Urine samples were aliquoted into cryotubes, frozen, and shipped on dry ice to a central laboratory for analysis (Clinical Chemistry Laboratory, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland). Both d- and l-lactate concentrations were normalised per mole creatinine (mmol lactate/mol creatinine).
Statistical methods
The sample size required to evaluate non-inferiority of the primary outcome (weight gain, g/day), based on a non-inferiority margin of −3.0 g/day and standard deviation (SD) for weight gain of 6.1 g/day (Barclay et al., 2003), was calculated as 79 infants per group. Since there were two primary comparisons (L. reuteri vs standard formula and B. lactis vs standard formula), Bonferroni’s adjustment was used to control the over-all type-1 error rate. With a type I error of 0.0125, a non-inferiority margin of −3 g/day, and SD of 6.1, a one-sided, two-sample z-test would require a sample size of 79 in each arm to detect non-inferiority with 80% power. Statistical analyses were performed using SAS Version 9.2 for Windows (Cary, North Carolina, US). The primary analysis was based on an intent-to-treat (ITT) approach. To compare the two probiotic formulas with the standard formula without probiotics with regard to weight gain from enrolment to 6 months of age (primary analysis), a mixed model with repeated visits was the choice of model because it provides a useful strategy to handle missing data due to dropout/loss-to-follow-up. The model was adjusted for sex, centre, and birth weight. The study was considered a success and non-inferiority was accepted if the lower bound of the two-sided 97.5% confidence interval (CI) of the mean difference did not reach −3 g/day for each of the 2 probiotic formula groups.

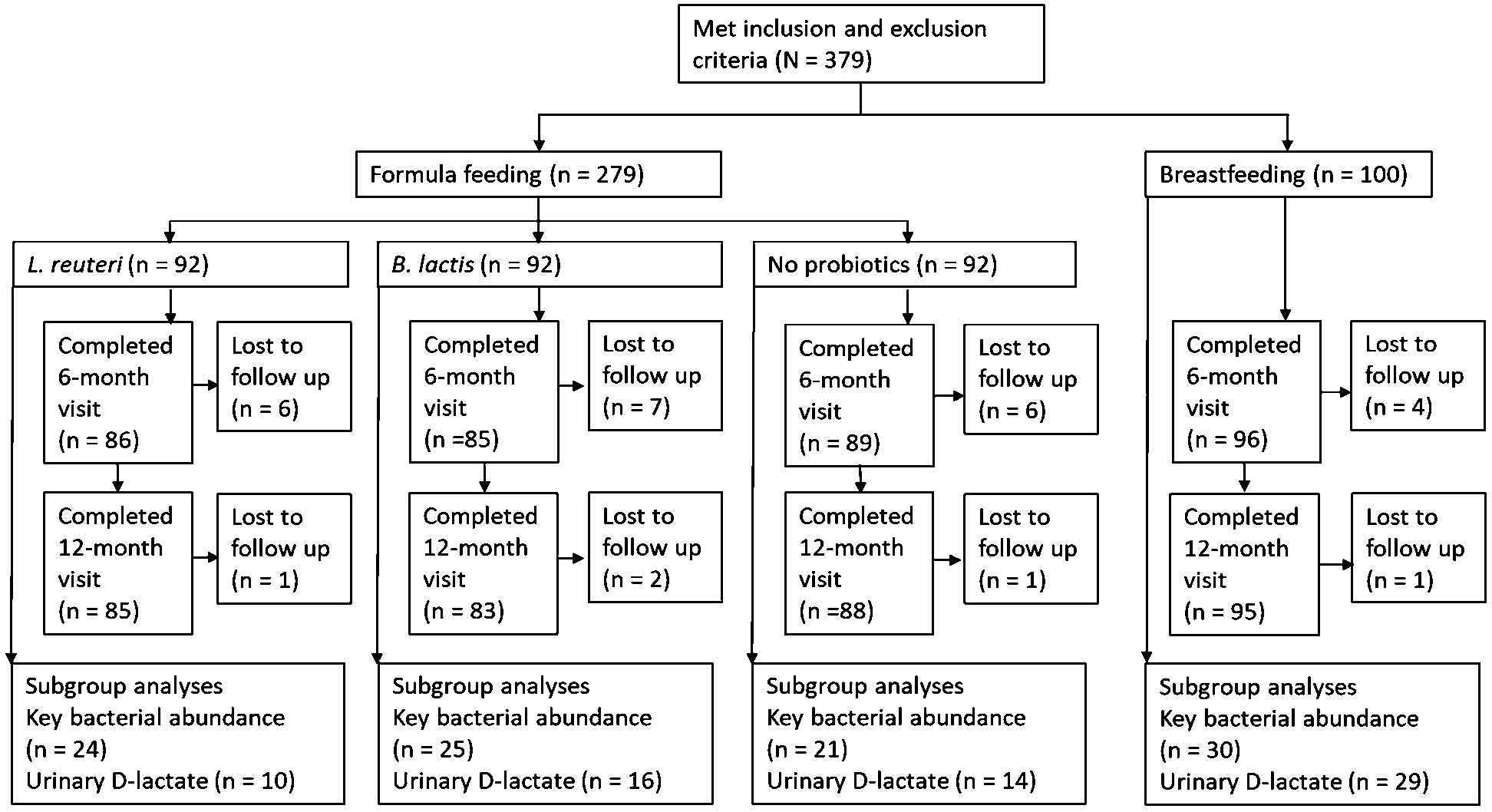
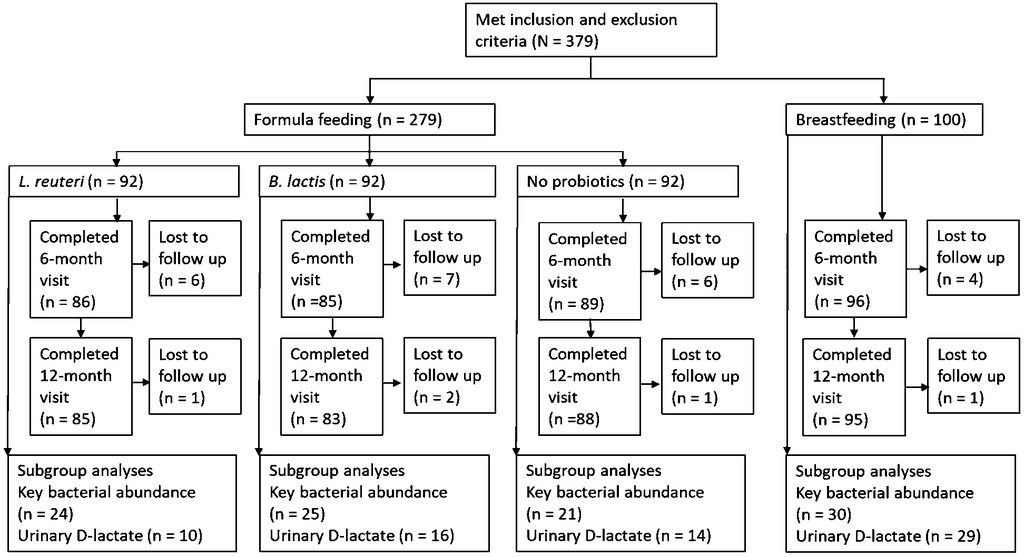
Subject disposition.
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
Differences in other anthropometric parameters between the two probiotic formulas and the standard formula were analysed in both the ITT population using a repeated measures model adjusted for sex, centre, and parameter value at birth. Stool frequency counts were aggregated to one total value of counts (i.e. all stools were reported for each subject and divided by the number of available days). Two-sided superiority testing for treatment differences between groups was assessed by Poisson regression on the stool count per day. The percentage of stools characterised as hard, formed, soft and liquid stools, was defined as number of stools with certain consistency divided by the total number of stools. For each stool consistency category, logistic regression was used to assess between-group superiority. Other GI tolerance symptoms such as spitting up, vomiting and sleeping data were assessed by Poisson regression, while flatulence and irritability/fussiness data were assessed by logistic regression.
Bacterial abundance in the fecal matter was expressed in log base 10 and was analysed by ANOVA. Parametric statistics were used and values below the detection limit were imputed to the detection limit value defined as 9.8 ∗ 1E5 bacteria/g of feces. Urinary lactate data was adjusted by log transformation (log base 10) and analysed using the same model as for bacterial abundance. Finally, the incidences of AEs were compared between groups by Chi-Square test. All gut microbiota data produced in the present study are available upon reasonable request to the authors.
3 Results
Study population
Two hundred seventy-nine mixed-fed infants were randomised to the L. reuteri-supplemented infant formula (L. reuteri,
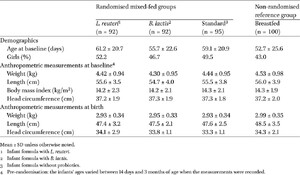
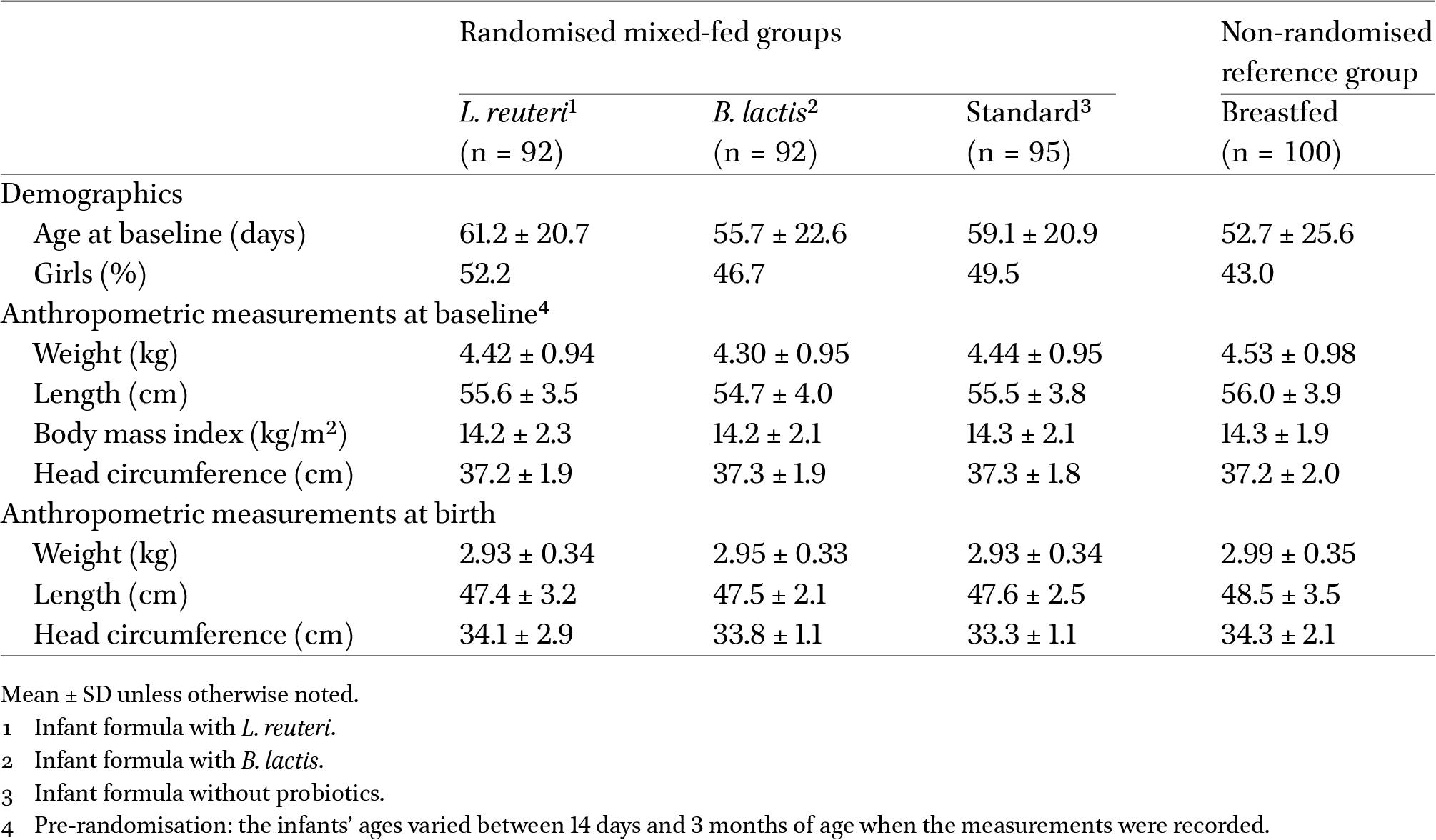
Baseline demographics and anthropometric characteristics
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
Weight gain and growth
The mean difference in weight gain between the two probiotic supplement groups and the standard group at 6 months of age was −0.378 g/day (97.5% CI, −1.541, 0.776) with L. reuteri and −1.724 g/day (97.5% CI, −2.845, −0.603) with B. lactis. Because the lower bound of the 97.5% CI in both comparisons was greater than −3 g/d, both test formulas demonstrated non-inferiority in weight gain velocity compared to the standard formula. The mean (SD) weight gain (g/day) was 22.73 (5.47), 20.93 (5.42) and 21.73 (5.42) with the L. reuteri-supplemented formula, B. lactis-supplemented formula, and the standard formula, respectively.
Body length, BMI, and head circumference were comparable among the 3 mixed-fed groups at 6 months and 12 months of age. Compared to the breastfed group, body length was slightly but significantly greater in each mixed-fed group (
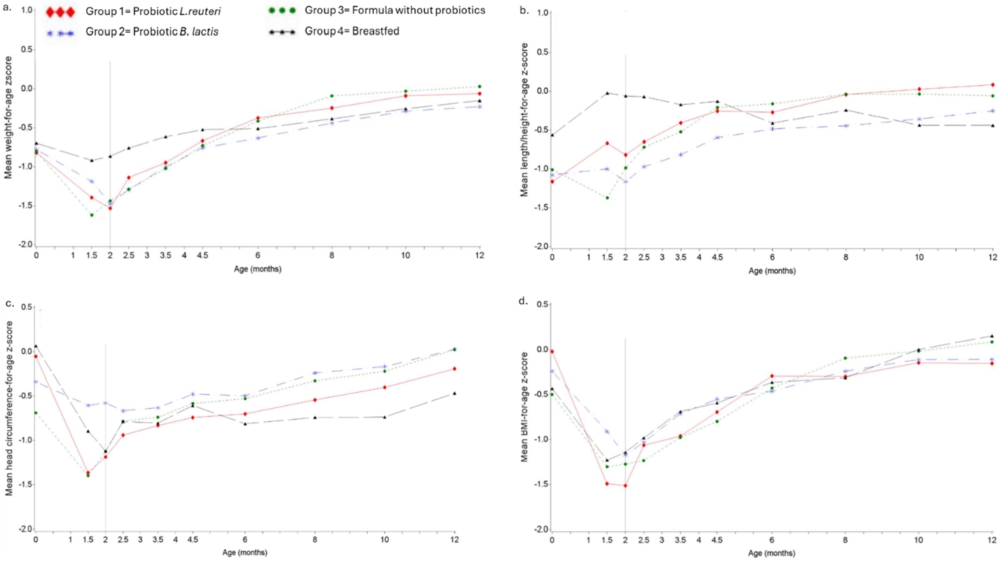
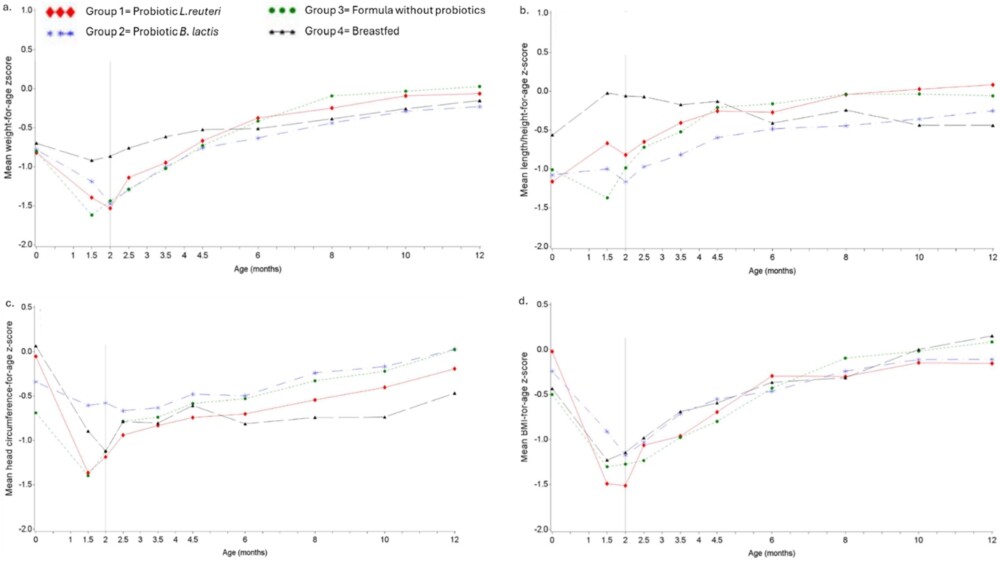
Mean weight-for-age Z-scores (a), length-for-age Z-scores (b), head circumference-for-age Z-scores (c), and BMI-for-age Z-scores (d) over time in infants up to 12 months of age. Mean values are raw values and are not adjusted for baseline values or sex. Vertical line represents mean age at initiation of study formula in randomised mixed-fed groups.
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
Changes in weight-for age, length-for age, and head circumference-for-age and BMI-for-age z-scores are shown in Figure 2. At 6 months of age, weight-for-age z-scores were slightly higher in the L. reuteri group compared to the B. lactis group (
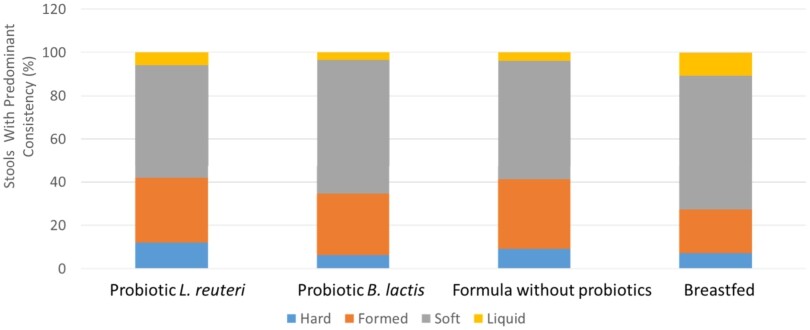
Percentage of stools with parent reported predominant stool consistency (hard, formed, soft, liquid) per group from baseline through through age 6 months.
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
Formula intake and digestive tolerance
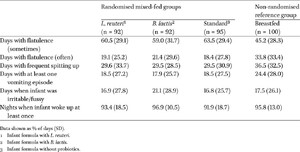
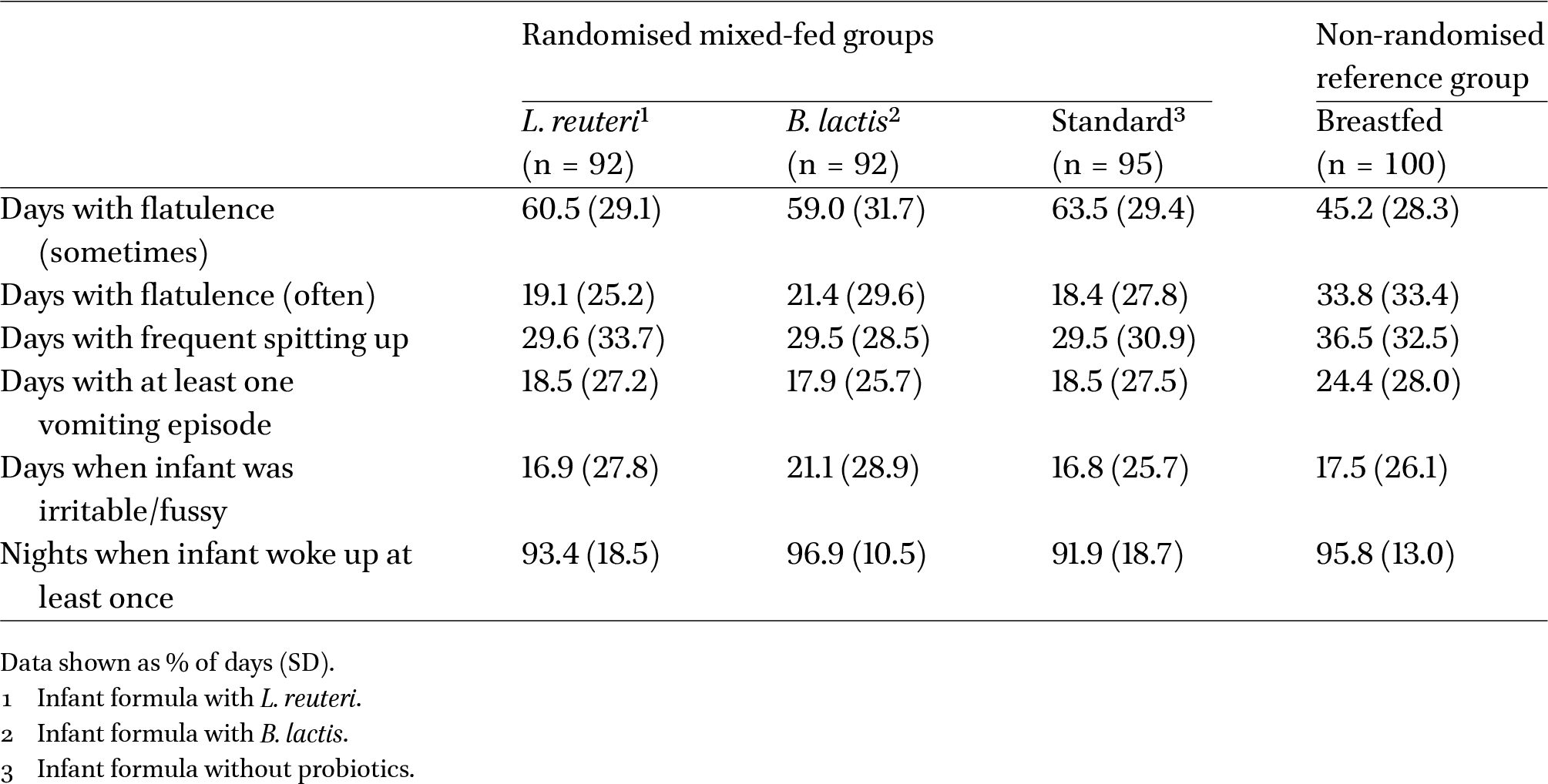
The overall number of breastfeeds per day were similar in the 3 formula groups (4.8 ± 2.6, 5.0 ± 2.4, and 5.0 ± 2.4 for the L. reuteri, B. lactis, and standard formula groups, respectively) and lower than the breastfed group (7.9 ± 0.31). Similarly, the overall reported formula intake per day was also similar in the 3 formula groups (505 ± 265, 487 ± 280, and 486 ± 241 ml/day for the L. reuteri, B. lactis, and standard formula groups, respectively). No formula intake was reported for the breastfed group until infants were aged 12 months, when average intake of 202 ± 243 ml/day was reported. Mean daily stool count was approximately 2 in all groups and approximately 80% to 90% of stools were either formed or soft (Figure 3). The number of days with parent reported frequent flatulence, frequent spitting up, or with at least 1 vomiting episode were similar in all feeding groups. Infants were reported by parents as irritable and fussy approximately 20% of the time in all groups, with no significant differences between groups (Table 2).
Parent reported GI tolerance related symptoms from randomisation to age six months
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
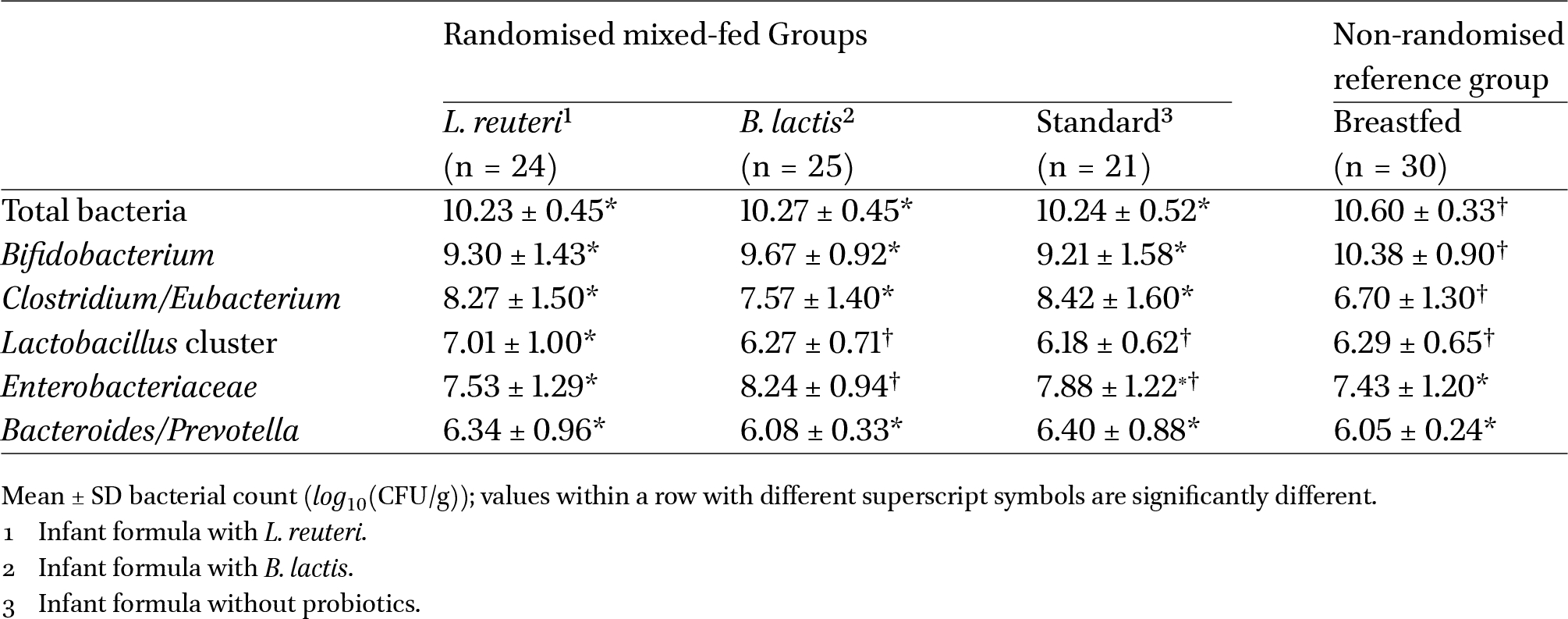
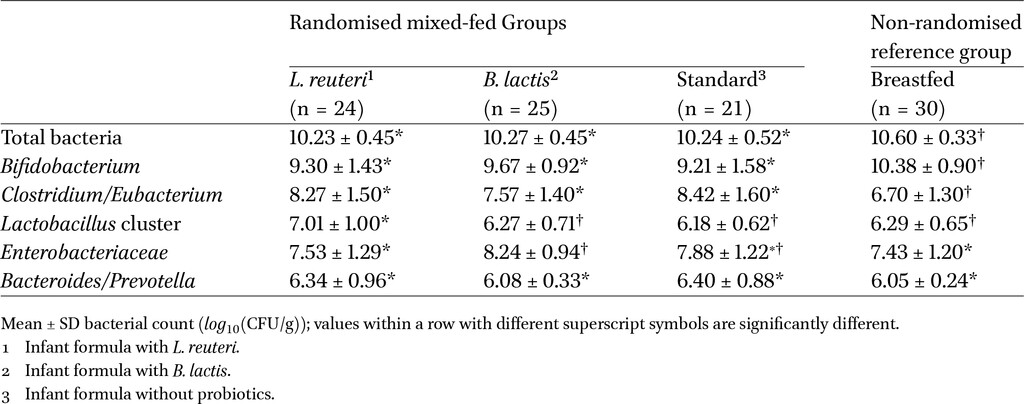
Abundance of bacteria in fecal matter in a subgroup of infants at 4.5 months of age
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
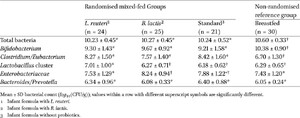
Abundance of key bacteria in fecal matter
The abundance of key bacteria in the fecal microbiota was evaluated in a subset of infants at 4.5 months of age (Table 3). There were no statistically significant differences between either the L. reuteri or the B. lactis group compared to the standard formula group with regard to total bacteria, bifidobacteria, or Clostridium, Enterobacteriaceae, and Bacteroides counts. Lactobacillus cluster counts (particularly L. reuteri and L. gasseri) were significantly higher in the L. reuteri group compared to infants fed B. lactis (
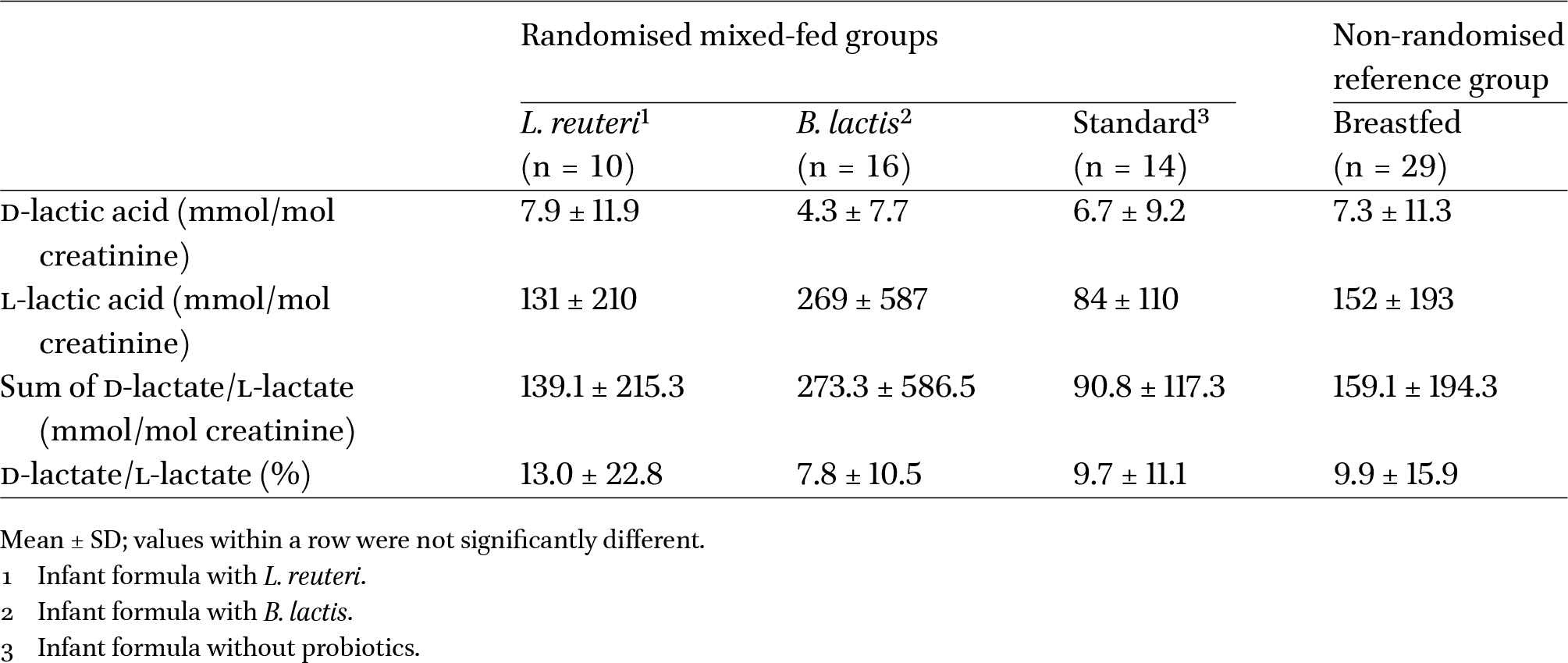
Urinary d-lactate
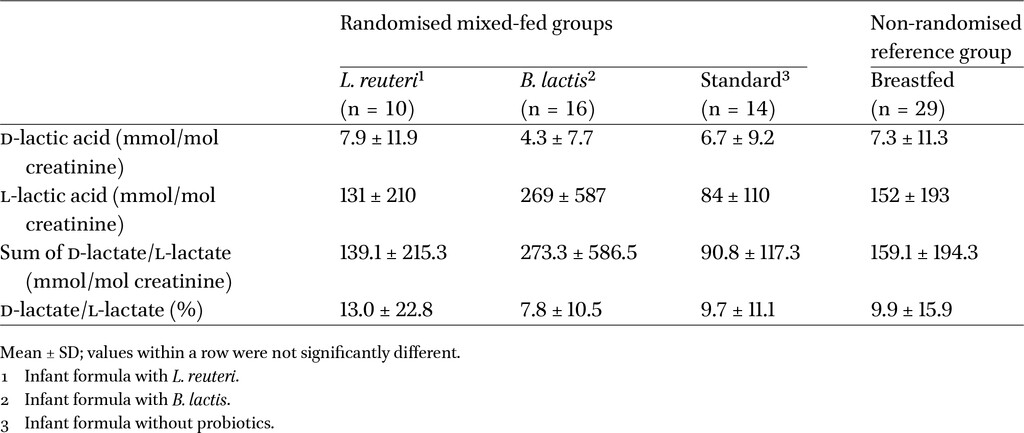
Urinary lactate levels, including d-lactate, l-lactate, percentage of d-lactate/l-lactate, and sum of d-lactate and l-lactate, were assessed in a subset of infants at approximately 2.5 months of age (2 months after the start of formula feeding in mixed-fed infants). No statistically significant differences were observed between any of the randomised formula groups or between the mixed-fed and the breastfed groups (Table 4).
Urinary D-lactate parameters in a subgroup of infants at 2.5 months of age
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
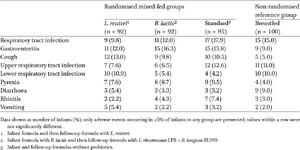
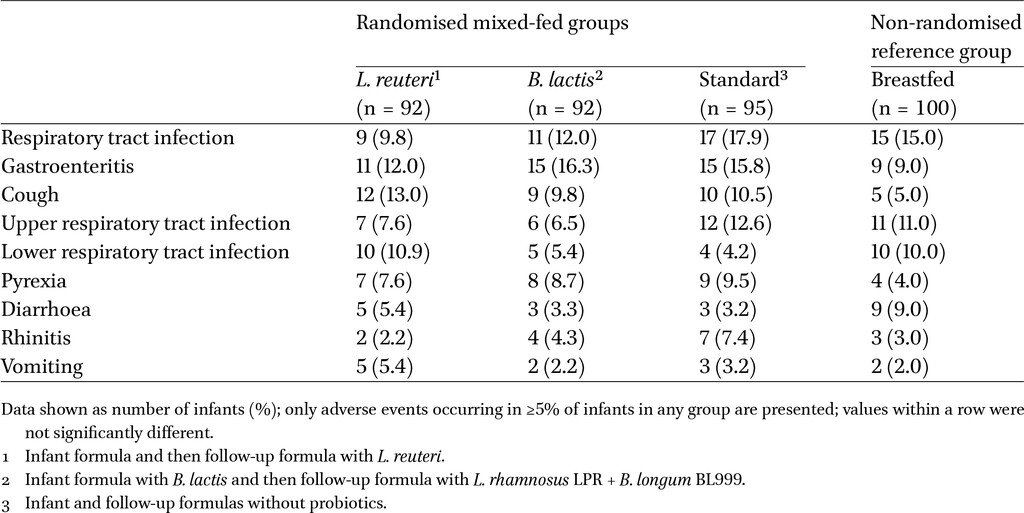
Adverse events occurring from randomisation until age 12 months
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00100
Adverse events
All infants who initiated formula (in the randomised groups) or entered into the study (breastfed groups) were included in the safety population. Treatment-emergent AEs occurred in 35 (38.0%) infants (110 events) in the L. reuteri group, 34 (37.0%) infants (100 events) in the B. lactis group, 41 (43.2%) infants (111 events) in the standard formula group, and 35 (35.0%) of infants (99 events) in the breastfed group. Serious treatment-emergent AEs were reported in 3 infants (3.3%; 3 events) in the L. reuteri group, 8 infants (8.7%; 9 events) in the B. lactis group, 3 infants (3.2%; 3 events) in the standard formula group, and 2 infants (2.0%; 2 events) in the breastfed group. Rates of the most commonly reported treatment-emergent AEs were generally similar among feeding groups (Table 5). In post-hoc analyses, the incidence of AEs between 6 and 12 months was compared between the L. reuteri group and controls. Children in the control group had a higher likelihood of AEs gastroenteritis (OR 4.29 (1.12-18.24),
4 Discussion
In this study, infant growth as assessed by mean weight gain per day in infants assigned to an infant formula supplemented with L. reuteri or B. lactis was non-inferior to the standard infant formula without probiotic supplementation.
Analysis of secondary growth outcomes based on the WHO Standards demonstrated no statistically significant differences in any of the z-score values for growth parameters (including z-scores for weight-for-age, length-for-age, and head circumference-for-age) between either of the probiotic formula groups and the standard formula group when infants were 6 or 12 months of age. However, compared to breastfed infants, z-scores at 12 months of age for weight-for-age, length-for-age and head circumference-for-age were significantly higher in all the mixed-fed groups. Interestingly, all study groups, including the breastfed reference group, grew faster during the study period 9 weeks to 6 months compared to the WHO standard. According to the WHO Standards, mean weight gain during this interval is, on average, 18.33 g/day. Mean weight gain was higher than this WHO standard in all 4 groups, with a difference of 4.15 g/day observed in the L. reuteri group (
Infant formulas with either L. reuteri or B. lactis supplementation were well tolerated. According to physicians’ reports, the incidence of AEs in infants in either probiotic group was comparable to the incidence in the standard formula group. Parent-reported stool characteristics and GI symptoms assessed up to 6 months of age were similar among all three formula groups. In addition, urinary lactate levels were comparable in all study groups, including the breastfed reference group, at 2.5 months of age. An increase in d-lactate-producing bacteria in the colon can lead to d-lactate acidosis, which is associated with neurological impairment (Kowlgi and Chhabra, 2015); thus, urinary d-lactate can be used as a safety biomarker for trials of infant formula supplemented with probiotics (Sanders et al., 2010). Urinary d-lactate values for individual subjects remained entirely within ranges previously reported in healthy infants (Haschke-Becher et al., 2000; 2008), and well below the values associated with d-lactate excess (e.g. approx. 60 mmol/mol creatinine (Bongaerts et al., 2000)). It is also worth noting that, in a subset of infants at 4.5 months of age, a significantly higher stool lactobacilli count was observed in the L. reuteri formula group vs the standard formula group and the breastfed group. This finding indicates that supplementation with L. reuteri may help promote a healthy gut microbiome.
The safety and tolerability of L. reuteri supplementation in our trial was consistent with findings from two earlier studies evaluating the safety of infant formulas containing L. reuteri (Lee Le et al., 2015; Papagaroufalis et al., 2014). In a previous study of 88 healthy full term newborns who were randomly assigned to an infant formula with L. reuteri or a control formula without probiotics (Papagaroufalis et al., 2014), all anthropometric measurements and safety parameters up to six months were comparable between the two formula groups. Further, Bifidobacterium and lactobacilli were detected more frequently in the L. reuteri group vs control (Papagaroufalis et al., 2014). Although we did not observe a higher fecal Bifidobacterium abundance in the present study, this may be due to our inclusion of mixed-fed infants versus exclusively formula-fed infants studied by Papagaroufalis et al. (2014), which may have limited our ability to detect differences between groups.
Various studies involving a collective total of more than 1,000 infants with L. reuteri doses as high as 1.2 × 109 CFU/day have consistently demonstrated the safety and tolerability of L. reuteri supplementation (Abrahamsson et al., 2009; Connolly et al., 2005; Indrio et al., 2011; Papagaroufalis et al., 2014; Savino et al., 2007; 2010; 2018; Tyrsin et al., 2024; Weizman et al., 2005). The totality of evidence demonstrates the safety and suitability of supplementing infants with the probiotic L. reuteri in supporting normal infant growth. Now with this study, we show safety and suitability at a concentration consistent with the estimated daily intake of L. reuteri from infant formula feeding.
B. lactis is one of the most extensively studied probiotic bacteria in infant nutrition. Its safety and tolerability are well established, both in healthy infants and toddlers and in at risk groups such as preterm infants and infants from HIV positive mothers (Steenhout et al., 2009; Tremblay et al., 2023). An independent safety evaluation by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition concluded that B. lactis, alone or in combination, supports normal growth in healthy term infants and is not associated with adverse outcomes (Braegger et al., 2011). The beneficial effects of B. lactis supplementation that have been reported in previous trials are numerous, and include an increase in the bifidobacteria in the gut microbiota, as well as reduced incidence of diarrhoea, rotavirus shedding, upper respiratory tract infections, diaper rash, and hard stools, and improved immune response (Chen et al., 2024; Dekker et al., 2022; Fukushima et al., 1998; Haschke et al., 1998; Hertiš Petek et al., 2022; Holscher et al., 2012; Langhendries et al., 1995; Phuapradit et al., 1999; Saavedra et al., 1994; 1998). In the present study, microbiota profile and GI tolerance in the B. lactis and standard formula groups were generally similar, perhaps due to the inclusion of mixed-fed infants (since breastmilk is also a strong influence on these endpoints).
One strength of the study is the number and location of the study sites (five centres, each in a geographically distinct region of India), which help to support the generalisability of these results to the Indian infant population. Another strength is the inclusion of mixed-fed infants, a population that is often excluded from infant formula trials even though many mothers introduce formula feeding as they prepare to wean or as maternity leave ends. One limitation of the study was the use of fluorescent in situ hybridisation, which is a less sensitive methodology for assessing presence of bacteria in fecal microbiota and their abundance compared to more modern techniques. Another limitation was the lack of assessment of gut microbiota at 12 months of age, which could have allowed evaluation of the effect of probiotic enrichment of the study follow-up formulas.
5 Conclusions
The results from this trial have demonstrated that infant formulas with L. reuteri or B. lactis compared with the same formula without probiotics promote adequate weight gain (g/day) in infants up to 6 months of age. The primary growth data, in conjunction with the growth outcomes based on the WHO Standards data (i.e. z-score values for growth parameters) during the entire 12-month study period, also demonstrate that follow-up formulas with L. reuteri or L. rhamnosus LPR + B. longum BL999, respectively, fed from 7 to 12 months of age support age-appropriate normal infant growth. These findings confirm the results of similar evaluations of infant formulas supplemented with probiotics in different geographic locations and populations (Gibson et al., 2009; Lee Le et al., 2015; Papagaroufalis et al., 2014; Soh et al., 2009; Weizman et al., 2005). Further, a significantly higher lactobacilli count in the L. reuteri formula group vs all other study groups, along with Enterobacteriaceae and Bacteroides/Prevotella counts that were similar to those of breastfed infants, indicate that supplementation with L. reuteri may help promote a healthy gut microbiome.
Rates of reported AEs with either the L. reuteri-supplemented formula or the B. lactis supplemented formula were comparable to those seen with both the standard infant formula and the breastfed reference group during the entire 12-month study period. The incidences of parent-reported GI symptoms such as spitting-up, vomiting, and irritability/fussiness were also similar among the three mixed-fed groups and comparable to those reported in the breastfed group. Consequently, this study confirms that infant formulas supplemented with probiotics L. reuteri or B. lactis are safe, well tolerated, and support normal infant growth in an Indian infant population.
Corresponding author; e-mail: nicholaspaul.hays@rd.nestle.com
Current address: TechMed Consulting Services, Lausanne, Switzerland.
Acknowledgements
The authors thank the research staff at each institution and the families who volunteered to participate. We also thank Emilie Darcillon for assistance with trial management and Dominik Grathwohl, Mickaël Hartweg, Bridget-Anne Kirwan and Emille Perrin for assistance with statistical analysis. We thank Hanne Tytgat for scientific review and Sophie Pecquet for assistance with manuscript preparation.
Authors’ contribution
MM, RA, UV and SG conceived and designed the study. MM, RA, and UV recruited study participants and supervised data collection. All authors jointly contributed to analysis and interpretation of data. AP and NPH developed the first draft of the manuscript, with editorial support provided by Cooper Johnson Communications, LLC, funded by Nestlé. All authors reviewed manuscript drafts and approved the final version.
Conflict of interest
APJ and NPH employees of Nestlé. SG was employed by Nestle at the time of study conduct.
Funding
The study was funded by Société des Produits Nestlé S.A. (previously Nestec Ltd). Co-authors employed by the funding body were involved in designing the study, data analysis and interpretation, and writing the manuscript.
Trial registration
CTRI/2010/091/001111 (Clinical Trials Registry – India; www.ctri.nic.in)
References
Abrahamsson, T.R., Jakobsson, T., Bottcher, M.F., Fredrikson, M., Jenmalm, M.C., Bjorksten, B. and Oldaeus, G., 2007. Probiotics in prevention of IgE-associated eczema: a double-blind, randomized, placebo-controlled trial. Journal of Allergy and Clinical Immunology 119: 1174-1180. https://doi.org/10.1016/j.jaci.2007.01.007
Abrahamsson, T.R., Sinkiewicz, G., Jakobsson, T., Fredrikson, M. and Bjorksten, B., 2009. Probiotic lactobacilli in breast milk and infant stool in relation to oral intake during the first year of life. Journal of Pediatric Gastroenterology and Nutrition 49: 349-354. https://doi.org/10.1097/MPG.0b013e31818f091b
Baglatzi, L., Gavrili, S., Stamouli, K., Zachaki, S., Favre, L., Pecquet, S., Benyacoub, J. and Costalos, C., 2016. Effect of infant formula containing a low dose of the probiotic Bifidobacterium lactis CNCM I-3446 on immune and gut functions in C-section delivered babies: a pilot study. Clinical Medicine Insights: Pediatrics 10: 11-19. https://doi.org/10.4137/CMPed.S33096
Barclay, D., Puccio, G., Fazzolari-Nesci, A., Giammanco, A., Räihä, N., Carrie-Fässier, A., Brown, C., Chauffard, F., Grathwohl, D., Hager, C., Haschke, F. and Endres, W., 2003. Growth and tolerance of a whey-based starter infant formula with enhanced protein efficiency and containing pro-, pre-, or synbiotics: a randomized controlled trial in term infants. Journal of Pediatric Gastroenterology and Nutrition 37: 388.
Berseth, C.L., Yeiser, M., Harris, C.L., Kinnaman, J.N., Lappin, V., Wampler, J.L., Zhuang, W. and Vanderhoof, J., 2024. Infant formula with added Lacticaseibacillus rhamnosus GG supported adequate growth and was well tolerated in healthy term infants: a randomized controlled trial. Frontiers in Pediatrics 12: 1456607. https://doi.org/10.3389/fped.2024.1456607
Bongaerts, G., Bakkeren, J., Severijnen, R., Sperl, W., Willems, H., Naber, T., Wevers, R., van Meurs, A. and Tolboom, J., 2000. Lactobacilli and acidosis in children with short small bowel. Journal of Pediatric Gastroenterology and Nutrition 30: 288-293.
Braegger, C., Chmielewska, A., Decsi, T., Kolacek, S., Mihatsch, W., Moreno, L., Piescik, M., Puntis, J., Shamir, R., Szajewska, H., Turck, D., van Goudoever, J. and ESPGHAN Committee on Nutrition, 2011. Supplementation of infant formula with probiotics and/or prebiotics: a systematic review and comment by the ESPGHAN committee on nutrition. Journal of Pediatric Gastroenterology and Nutrition 52: 238-250. https://doi.org/10.1097/MPG.0b013e3181fb9e80
Chen, K., Jin, S., Ma, Y., Cai, L., Xu, P., Nie, Y., Luo, L., Yu, Q., Shen, Y., Zhou, Z. and Liu, C., 2024. Adjudicative efficacy of Bifidobacterium animalis subsp. lactis BLa80 in treating acute diarrhea in children: a randomized, double-blinded, placebo-controlled study. European Journal of Clinical Nutrition 78: 501-508. https://doi.org/10.1038/s41430-024-01428-6
Chouraqui, J.P., Van Egroo, L.D. and Fichot, M.C., 2004. Acidified milk formula supplemented with Bifidobacterium lactis: impact on infant diarrhea in residential care settings. Journal of Pediatric Gastroenterology and Nutrition 38: 288-292.
Connolly, E., Abrahamsson, T. and Bjorksten, B., 2005. Safety of D-lactic acid producing bacteria in the human infant. Journal of Pediatric Gastroenterology and Nutrition 41: 489-492.
Dekker, J., Quilter, M. and Qian, H., 2022. Comparison of two probiotics in follow-on formula: Bifidobacterium animalis subsp. lactis HN019 reduced upper respiratory tract infections in Chinese infants. Beneficial Microbes 13: 341-354. https://doi.org/10.3920/bm2022.0041
Duar, R.M., Kyle, D. and Casaburi, G., 2020. Colonization resistance in the infant gut: the role of B. infantis in reducing pH and preventing pathogen growth. High-Throughput 9. https://doi.org/10.3390/ht9020007
Fukushima, Y., Kawata, Y., Hara, H., Terada, A. and Mitsuoka, T., 1998. Effect of a probiotic formula on intestinal immunoglobulin A production in healthy children. International Journal of Food Microbiology 42: 39-44.
Gibson, G.R. and Roberfroid, M.B., 1995. Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. The Journal of Nutrition 125: 1401-1412.
Gibson, R.A., Barclay, D., Marshall, H., Moulin, J., Maire, J.C. and Makrides, M., 2009. Safety of supplementing infant formula with long-chain polyunsaturated fatty acids and Bifidobacterium lactis in term infants: a randomised controlled trial. British Journal of Nutrition 101: 1706-1713. https://doi.org/10.1017/S0007114508084080
Haschke-Becher, E., Baumgartner, M. and Bachmann, C., 2000. Assay of D-lactate in urine of infants and children with reference values taking into account data below detection limit. Clinica Chimica Acta 298: 99-109.
Haschke-Becher, E., Brunser, O., Cruchet, S., Gotteland, M., Haschke, F. and Bachmann, C., 2008. Urinary D-lactate excretion in infants receiving Lactobacillus johnsonii with formula. Annals of Nutrition & Metabolism 53: 240-244. https://doi.org/10.1159/000185642
Haschke, F., Wang, W., Ping, G., Varavithya, W., Podhipak, A., Rochat, F., Link-Amster, H., Pfeifer, A., Diallo-Ginstl, E. and Steenhout, P., 1998. Clinical trials prove the safety and efficacy of the probiotic strain Bifidobacterium Bb12 in follow-up formula and growing-up milks. Monatsschrift Kinderheilkunde 146: S26-S30. https://doi.org/10.1007/PL00014763
Hascoet, J.M., Hubert, C., Rochat, F., Legagneur, H., Gaga, S., Emady-Azar, S. and Steenhout, P.G., 2011. Effect of formula composition on the development of infant gut microbiota. Journal of Pediatric Gastroenterology and Nutrition 52: 756-762. https://doi.org/10.1097/MPG.0b013e3182105850
Hertiš Petek, T., Petek, M., Petek, T. and Marčun Varda, N., 2022. Emerging links between microbiome composition and skin immunology in diaper dermatitis: a narrative review. Children 9. https://doi.org/10.3390/children9010112
Holscher, H.D., Czerkies, L.A., Cekola, P., Litov, R., Benbow, M., Santema, S., Alexander, D.D., Perez, V., Sun, S., Saavedra, J.M. and Tappenden, K.A., 2012. Bifidobacterium lactis Bb12 enhances intestinal antibody response in formula-fed infants: a randomized, double-blind, controlled trial. JPEN Journal of Parenteral and Enteral Nutrition 36: 106S-117S. https://doi.org/10.1177/0148607111430817
Indrio, F., Riezzo, G., Raimondi, F., Bisceglia, M., Cavallo, L. and Francavilla, R., 2008. The effects of probiotics on feeding tolerance, bowel habits, and gastrointestinal motility in preterm newborns. The Journal of Pediatrics 152: 801-806. https://doi.org/10.1016/j.jpeds.2007.11.005
Indrio, F., Riezzo, G., Raimondi, F., Bisceglia, M., Filannino, A., Cavallo, L. and Francavilla, R., 2011. Lactobacillus reuteri accelerates gastric emptying and improves regurgitation in infants. European Journal of Clinical Investigation 41: 417-422. https://doi.org/10.1111/j.1365-2362.2010.02425.x
Isolauri, E., Arvola, T., Sutas, Y., Moilanen, E. and Salminen, S., 2000. Probiotics in the management of atopic eczema. Clinical and Experimental Allergy 30: 1604-1610.
Kowlgi, N.G. and Chhabra, L., 2015. D-lactic acidosis: an underrecognized complication of short bowel syndrome. Gastroenterology Research and Practice 2015: 476215. https://doi.org/10.1155/2015/476215
Langhendries, J.P., Detry, J., Van Hees, J., Lamboray, J.M., Darimont, J., Mozin, M.J., Secretin, M.C. and Senterre, J., 1995. Effect of a fermented infant formula containing viable bifidobacteria on the fecal flora composition and pH of healthy full-term infants. Journal of Pediatric Gastroenterology and Nutrition 21: 177-181.
Lee Le, Y., Bharani, R., Biswas, A., Lee, J., Tran, L.A., Pecquet, S. and Steenhout, P., 2015. Normal growth of infants receiving an infant formula containing Lactobacillus reuteri, galacto-oligosaccharides, and fructo-oligosaccharide: a randomized controlled trial. Maternal Health, Neonatology and Perinatology 1: 9. https://doi.org/10.1186/s40748-015-0008-3
Lundeen, E.A., Stein, A.D., Adair, L.S., Behrman, J.R., Bhargava, S.K., Dearden, K.A., Gigante, D., Norris, S.A., Richter, L.M., Fall, C.H., Martorell, R., Sachdev, H.S. and Victora, C.G., 2014. Height-for-age z scores increase despite increasing height deficits among children in 5 developing countries. The American Journal of Clinical Nutrition 100: 821-825. https://doi.org/10.3945/ajcn.114.084368
Odiase, E., Frank, D.N., Young, B.E., Robertson, C.E., Kofonow, J.M., Davis, K.N., Berman, L.M., Krebs, N.F. and Tang, M., 2023. The gut microbiota differ in exclusively breastfed and formula-fed United States infants and are associated with growth status. The Journal of Nutrition 153: 2612-2621. https://doi.org/10.1016/j.tjnut.2023.07.009
Papagaroufalis, K., Fotiou, A., Egli, D., Tran, L.A. and Steenhout, P., 2014. A randomized double blind controlled safety trial evaluating D-lactic acid production in healthy infants fed a Lactobacillus reuteri-containing formula. Nutrition and Metabolic Insights 7: 19-27. https://doi.org/10.4137/NMI.S14113
Phuapradit, P., Varavithya, W., Vathanophas, K., Sangchai, R., Podhipak, A., Suthutvoravut, U., Nopchinda, S., Chantraruksa, V. and Haschke, F., 1999. Reduction of rotavirus infection in children receiving bifidobacteria-supplemented formula. Journal of the Medical Association of Thailand 82: S43-S48.
Radke, M., Picaud, J.C., Loui, A., Cambonie, G., Faas, D., Lafeber, H.N., de Groot, N., Pecquet, S.S., Steenhout, P.G. and Hascoet, J.M., 2017. Starter formula enriched in prebiotics and probiotics ensures normal growth of infants and promotes gut health: a randomized clinical trial. Pediatric Research 81: 622-631. https://doi.org/10.1038/pr.2016.270
Saavedra, J., Abi-Hanna, A., Moore, N. and Yolken, R., 1998. Effect of long term consumption of infant formulas with Bifidobacteria (B) and S. Thermophillus (ST) on stool patterns and diaper rash in infants. In: Annual meeting of the North American Society for Pediatric Gastroenterology and Nutrition, Orlando, Florida, pp. 483.
Saavedra, J.M., Bauman, N.A., Oung, I., Perman, J.A. and Yolken, R.H., 1994. Feeding of Bifidobacterium bifidum and Streptococcus thermophilus to infants in hospital for prevention of diarrhoea and shedding of rotavirus. The Lancet 344: 1046-1049.
Saji, A., Baby, J., Antony, P., Sinha, S., Bandyopadhyay, S., Jose, J.K., Kurpad, A.V. and Thomas, T., 2024. Growth dynamics of Indian infants using latent trajectory models in pooled survey datasets. Frontiers in Public Health 12: 1474222. https://doi.org/10.3389/fpubh.2024.1474222
Sanders, M.E., Akkermans, L.M., Haller, D., Hammerman, C., Heimbach, J., Hörmannsperger, G., Huys, G., Levy, D.D., Lutgendorff, F., Mack, D., Phothirath, P., Solano-Aguilar, G. and Vaughan, E., 2010. Safety assessment of probiotics for human use. Gut Microbes 1: 164-185. https://doi.org/10.4161/gmic.1.3.12127
Savino, F., Cordisco, L., Tarasco, V., Palumeri, E., Calabrese, R., Oggero, R., Roos, S. and Matteuzzi, D., 2010. Lactobacillus reuteri DSM 17938 in infantile colic: a randomized, double-blind, placebo-controlled trial. Pediatrics 126: e526-e533. https://doi.org/10.1542/peds.2010-0433
Savino, F., Garro, M., Montanari, P., Galliano, I. and Bergallo, M., 2018. Crying time and RORγ/FOXP3 expression in Lactobacillus reuteri DSM17938-treated infants with colic: a randomized trial. The Journal of Pediatrics 192: 171-177.e171. https://doi.org/10.1016/j.jpeds.2017.08.062
Savino, F., Pelle, E., Palumeri, E., Oggero, R. and Miniero, R., 2007. Lactobacillus reuteri (American type culture collection strain 55730) versus simethicone in the treatment of infantile colic: a prospective randomized study. Pediatrics 119: e124-e130. https://doi.org/10.1542/peds.2006-1222
Shen, S.P., Lin, H.C., Chen, J.F., Wang, H.S., Huang, Y.Y., Hsia, K.C., Lin, J.H., Kuo, Y.W., Li, C.M., Hsu, Y.C., Tsai, S.Y. and Ho, H.H., 2024. Assessment of the safety and gut microbiota modulation ability of an infant formula containing Bifidobacterium animalis ssp. lactis CP-9 or Lactobacillus salivarius AP-32 and the effects of the formula on infant growth outcomes: insights from a four-month clinical study in infants under two months old. BMC Pediatrics 24: 840. https://doi.org/10.1186/s12887-024-05289-7
Shulman, R.J., Chichlowski, M., Orozco, F.G., Harris, C.L., Wampler, J.L., Bokulich, N.A. and Berseth, C.L., 2022. Infant behavioral state and stool microbiome in infants receiving Lactocaseibacillus rhamnosus GG in formula: randomized controlled trial. BMC Pediatrics 22: 580. https://doi.org/10.1186/s12887-022-03647-x
Soh, S.E., Aw, M., Gerez, I., Chong, Y.S., Rauff, M., Ng, Y.P., Wong, H.B., Pai, N., Lee, B.W. and Shek, L.P., 2009. Probiotic supplementation in the first 6 months of life in at risk Asian infants – effects on eczema and atopic sensitization at the age of 1 year. Clinical and Experimental Allergy 39: 571-578. https://doi.org/10.1111/j.1365-2222.2008.03133.x
Steenhout, P.G., Rochat, F. and Hager, C., 2009. The effect of Bifidobacterium lactis on the growth of infants: a pooled analysis of randomized controlled studies. Annals of Nutrition & Metabolism 55: 334-340. https://doi.org/10.1159/000248992
Stuebe, A., 2009. The risks of not breastfeeding for mothers and infants. Revue Obstétricale Et Gynécologique 2: 222-231.
Tremblay, A., Bronner, S. and Binda, S., 2023. Review and perspectives on Bifidobacterium lactis for infants’ and children’s health. Microorganisms 11. https://doi.org/10.3390/microorganisms11102501
Tyrsin, O.Y., Tyrsin, D.Y., Nemenov, D.G., Ruzov, A.S., Odintsova, V.E., Koshechkin, S.I. and D’Amico, L., 2024. Effect of Lactobacillus reuteri NCIMB 30351 drops on symptoms of infantile functional gastrointestinal disorders and gut microbiota in early infants: results from a randomized, placebo-controlled clinical trial. European Journal of Pediatrics 183: 2311-2324. https://doi.org/10.1007/s00431-024-05473-y
Underwood, M.A., Kalanetra, K.M., Bokulich, N.A., Lewis, Z.T., Mirmiran, M., Tancredi, D.J. and Mills, D.A., 2013. A comparison of two probiotic strains of bifidobacteria in premature infants. The Journal of Pediatrics 163: 1585-1591.e9 https://doi.org/10.1016/j.jpeds.2013.07.017
Urbanska, M. and Szajewska, H., 2014. The efficacy of Lactobacillus reuteri DSM 17938 in infants and children: a review of the current evidence. European Journal of Pediatrics 173: 1327-1337. https://doi.org/10.1007/s00431-014-2328-0
Weizman, Z., Asli, G. and Alsheikh, A., 2005. Effect of a probiotic infant formula on infections in child care centers: comparison of two probiotic agents. Pediatrics 115: 5-9. https://doi.org/10.1542/peds.2004-1815
Yang, I., Corwin, E.J., Brennan, P.A., Jordan, S., Murphy, J.R. and Dunlop, A., 2016. The infant microbiome: implications for infant health and neurocognitive development. Nursing Research 65: 76-88. https://doi.org/10.1097/nnr.0000000000000133
Yao, Y., Cai, X., Ye, Y., Wang, F., Chen, F. and Zheng, C., 2021. The role of microbiota in infant health: from early life to adulthood. Frontiers in Immunology 12: 708472. https://doi.org/10.3389/fimmu.2021.708472





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}