Abstract
Irritable bowel syndrome (IBS) is faced by gastroenterologists daily, and probiotics are a potential therapeutic tool; however, there are no strain recommendations. This multicenter, real-world, single-arm, open-label study aims to assess a novel probiotic mixture’s effectiveness, safety, and patient satisfaction in patients with IBS. This study was conducted by 52 Italian gastroenterologists across 16 of the 21 Italian regions who enrolled patients with IBS (n = 1,098). Throughout the 8-week treatment (T1) period with a probiotic mixture (Lactobacillus paracasei 101/37 LMG P-17504, Lactobacillus plantarum 14D CECT 4528, Bifidobacterium breve Bbr8 LMG P-17501, Bifidobacterium breve BL10 LMG P-17500, and Bifidobacterium animalis ssp. lactis Bi1 LMG P-17502), participants completed a questionnaire to evaluate IBS symptoms at baseline, at the end of treatment, and after one-month follow-up (T2). The primary outcome was the progress of abdominal pain and bloating according with a 5-point Likert scale, (0 absence and 5 highly intense symptoms) and treatment success was defined as a change towards categories of lower IBS severity for abdominal pain and/or bloating. Treatment success for abdominal pain and bloating was achieved in 73% and 81.9% at T1 and 68% and 73.1% at T2, respectively. The probiotic was associated with significantly reducing abdominal pain and bloating at T1 and T2 (P < 0.001). Patients with regular bowel movements increased to 68.5% at T1 and 68.7% at T2, respectively (P < 0.001). Patients reporting that IBS did not affect their daily life increased from 1.8% at entry to 22.7% at T1 and 41.6% at T2 (P < 0.001). This real-world, single-arm, open-label study showed that an 8-week treatment with a novel probiotic mixture is effective, safe, well tolerated, and can improve patients’ social lives during and after treatment. Future randomised placebo-controlled studies are necessary to validate these findings.
The trial is registered at www.ClinicalTrials.gov (NCT06610149).
1 Introduction
Irritable bowel syndrome (IBS) is a chronic digestive disorder characterised by chronic abdominal pain and disturbances in bowel movements. It affects around 4% to 10% of the general population (Sperber et al., 2021). IBS may significantly impact quality of life, particularly in its most severe manifestations, which account for around 25% of cases (Drossman et al., 2011).
IBS involves multiple factors that are not entirely understood, and recent studies have indicated that various mechanisms contribute to its development. These mechanisms include disruptions in the communication between the brain and the gut, interactions between the gut microbiota, the intestinal barrier, visceral hypersensitivity, low-grade gut inflammation, psychological disturbances, and genetic factors (Black and Ford, 2020). These events result in a loss of tolerance towards the gut flora and a prolonged and improper inflammatory reaction. As per the Rome IV diagnostic criteria, IBS is characterised by recurrent abdominal pain occurring at least once a week during the past three months. This pain is accompanied by two or more of the following criteria: (i) related to defecation, (ii) a change in frequency of stools, and (iii) a change in form (appearance) of stools. IBS is often accompanied by supplementary signs such as abdominal bloating, excessive flatulence, episodes of diarrhoea, and periods of constipation. The Rome IV diagnostic categorises individuals with IBS into four subtypes based on the intensity, duration, and rank of their symptoms: diarrhoea-predominant (IBS-D), constipation-predominant (IBS-C), mixed (IBS-M), and unclassified (IBS-U) (Lacy and Patel, 2017).
Interventions that impact the microbiota and the gut barrier offer a potentially effective strategy for managing IBS. Studies have shown that certain strains of probiotic bacteria can effectively regulate the microbiota, enhance the integrity of the gut barrier, and thereby decrease gut inflammation (Chlebicz-Wójcik and Śliżewska, 2021). Randomised controlled trials (RCTs) have demonstrated that multiple probiotic strains effectively reduce the frequency and severity of symptoms associated with IBS. However, there is no recommendation for a particular strain (Guarino and Canani, 2016).
IBS management should be based on a multifaceted approach targeting diet, behaviour, symptom relief, and quality of life (Lacy et al., 2021). Medications may be helpful, but they are very rarely resolutive and may induce adverse events. Therefore, non-pharmacological remedies may be valuable in managing IBS patients (Leahy and Epstein, 2001).
Our group has recently demonstrated the positive effect of a multispecies probiotic supplementation in improving the severity of IBS-type symptoms in patients with celiac disease adherent to a strict gluten-free diet. Evidence from this RCT has proven the strain’s efficacy (versus placebo) in alleviating the typical symptoms (abdominal pain, bloating, passage of gas, and bowel dysfunction) and in reducing disease severity even six weeks after the discontinuation of probiotics (Francavilla et al., 2019), and this was the reason for testing this combination in the adult population affected by IBS.
IBS is a highly individualised condition, with symptoms and signs that are easily affected by variables such as food, psychosocial problems, and comorbidities that need to be considered in the study design. In RCTs, these variables are rigorously controlled, and the use of real-world evidence should be seen as a valuable tool supporting RCTs’ findings. As a result, well-designed trials allow RCT evidence to be used in the real world, which is crucial for effectiveness, safety, tolerability, and patient satisfaction (Arlett et al., 2022).
This study aims to evaluate the efficacy and safety of a novel probiotic mixture in alleviating the symptoms of IBS in adults. We hypothesise that this probiotic mixture will significantly improve IBS symptoms compared to baseline, offering a potential new therapeutic option for managing this condition in real-world clinical settings.
2 Materials and methods
Study design
The study was conducted under the Helsinki Declaration and the ISO 14155 standard on Clinical Investigation of Medical Devices for Human Subjects – Good Clinical Practice and was approved by the institutional ethical committee (CET 46-2024; 29/12/2023). The full trial protocol can be accessed at www.ClinicalTrials.gov (identifier NCT06610149). All study participants provided written informed consent. Patients involved have received written and transparent information about the study’s design and aim and signed an informed consent.
This was a prospective, open-label, observational, post-market clinical study (IBSdammiil5). Participants who were diagnosed with IBS according to the Rome IV criteria (Drossman and Hasler, 2016) (aged 18 or over) were considered eligible for the study and enrolled between October 2022 and June 2023. Patients were required to experience recurrent abdominal pain at least once per week on average during the past three months associated with two or more of the following criteria: related to defecation, associated with a change in the frequency of stool, or the appearance of stool.
Seventy-five gastroenterologists across Italy were contacted, and 52 (69%) recruited patients. Gastroenterologists from all the Italian territory (16 of the 21 Italian regions) enrolled the participants among patients seeking treatment for their IBS. The gastroenterologists had the discretion to either prescribe or not prescribe the study product based on their assessment of whether it was a suitable treatment choice for the patient. Participants in the study were instructed to continue with their regular diet, exercise routines, smoking habits, and medications. The administration of antibiotics and any changes in treatment that could affect the microbiota, gut motility, or gastrointestinal symptoms (such as loperamide, rifaximin, antispasmodics, laxatives, and prokinetics) or the use of any additional probiotics throughout the treatment and follow-up period were not allowed and were considered reasons to exit the study. Each participant received an information letter outlining the study’s goals, design, and objective, and those who consented entered the study. During the initial consultation (T0), relevant patient information, such as gender, age, medical history, non-IBS related health issues, concurrent therapy, and disease features (including onset mode, length, transit sub-type, therapies, and underlying conditions), were collected. After that, participants completed an online questionnaire under the guidance of the gastroenterologist to input their IBS symptoms and the impact of IBS on their professional, private, and social situations.
Patients were instructed to consume one sachet daily of the study product for eight consecutive weeks. A second consultation with the gastroenterologist was planned at the end of the treatment period (week 8 – T1) and the last consultation, one month after treatment discontinuation (week 12 – T2).
Study product
The study product is a probiotic mixture containing five strains [Lactobacillus paracasei 101/37 LMG P-17504 (5 × 109 CFU), Lactobacillus plantarum 14D CECT 4528 (5 × 109 CFU), Bifidobacterium breve Bbr8 LMG P-17501 (3.4 × 109 CFU), Bifidobacterium breve BL10 LMG P-17500 (3.4 × 109 CFU), and Bifidobacterium animalis ssp. lactis Bi1 LMG P-17502 (3.4 × 109 CFU)] (Pentabiocel®, Noos, Rome, Italy). The formulation contains excipients such as maize starch hydroxypropyl methylcellulose. The product aims to treat symptoms associated with IBS, such as (constipation, diarrhoea, bloating, and flatulence).
Evaluations and outcomes
The study’s primary outcome was to evaluate the progress of abdominal pain and bloating before, at the end of treatment, and four weeks after discontinuation. The questionnaire utilised a 5-point Likert scale, where 0 represented the absence of symptoms, and 5 indicated the presence of highly intense symptoms. Treatment success was defined as a change towards categories of lower IBS severity for abdominal pain and/or bloating between inclusion (T0) and the end of the supplementation period (T1). Secondary endpoints were (a) days with pain (in the ten days preceding the time point), (b) daily number of bowel movements (<3; 1-3 daily; >3; (c) stool consistency (using the seven-point Bristol scale) and (d) need of an elimination diet. Other endpoints included evaluating the impact of IBS symptoms on the overall quality of life (anxiety when eating out and about one’s health), using a 4-point scale that ranged from ‘no impact’ to ‘serious impact’. Patients documented their treatment consumption in a daily report form. Safety was assessed by actively collecting and documenting any adverse events (AEs) reported by participants during treatment and follow-up. At each visit, patients were asked about the occurrence of any new or worsening symptoms, irrespective of their potential relationship to the study product. All AEs were recorded with details on onset, duration, severity, and outcome, and their relationship to the intervention was evaluated by the investigator. Although a formal standardised AE grading scale was not used, events were classified as mild, moderate, or severe according to clinical judgement. The general tolerability of the study product was evaluated by participants using a 6-point Likert scale, ranging from 1 (very good) to 6 (extremely bad).
Statistical analysis
Data were reported primarily using an intention-to-treat (ITT) analysis. A per-protocol (PP) analysis is reported in the tables. Descriptive data are presented as the mean ± SD for continuous variables and as frequency and percentage for categorical data. The distributions of categorical variables at the different time points were analysed using a generalised linear mixed model using multinominal logits. The results of the analyses for the intention to treat the population are presented. Statistical significance was set at P < 0.05. The original patient recruitment goal was as follows. A change towards categories of lower IBS severity (for both abdominal pain and/or bloating) is expected in at least 40% of the participants due to a placebo effect (Miller, 2014). Therefore, we determined that 815 individuals should be recruited to identify an impact ranging between 5 and 35%, using a two-tailed binomial test, a power of 95%, an alpha risk of 0.05 and a 10% drop-out rate. Calculation was based on ITT and PP analysis for treatment success and on ITT for all the remaining analysis. Cochran’s Q test, followed by Bonferroni-adjusted pairwise comparisons, was applied to determine the presence of statistically significant differences in the proportions of categorical data.
3 Results
Demographic and clinical characteristics

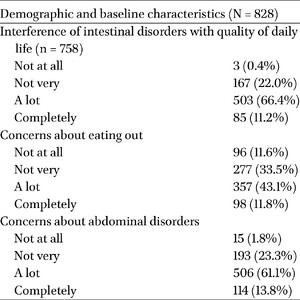
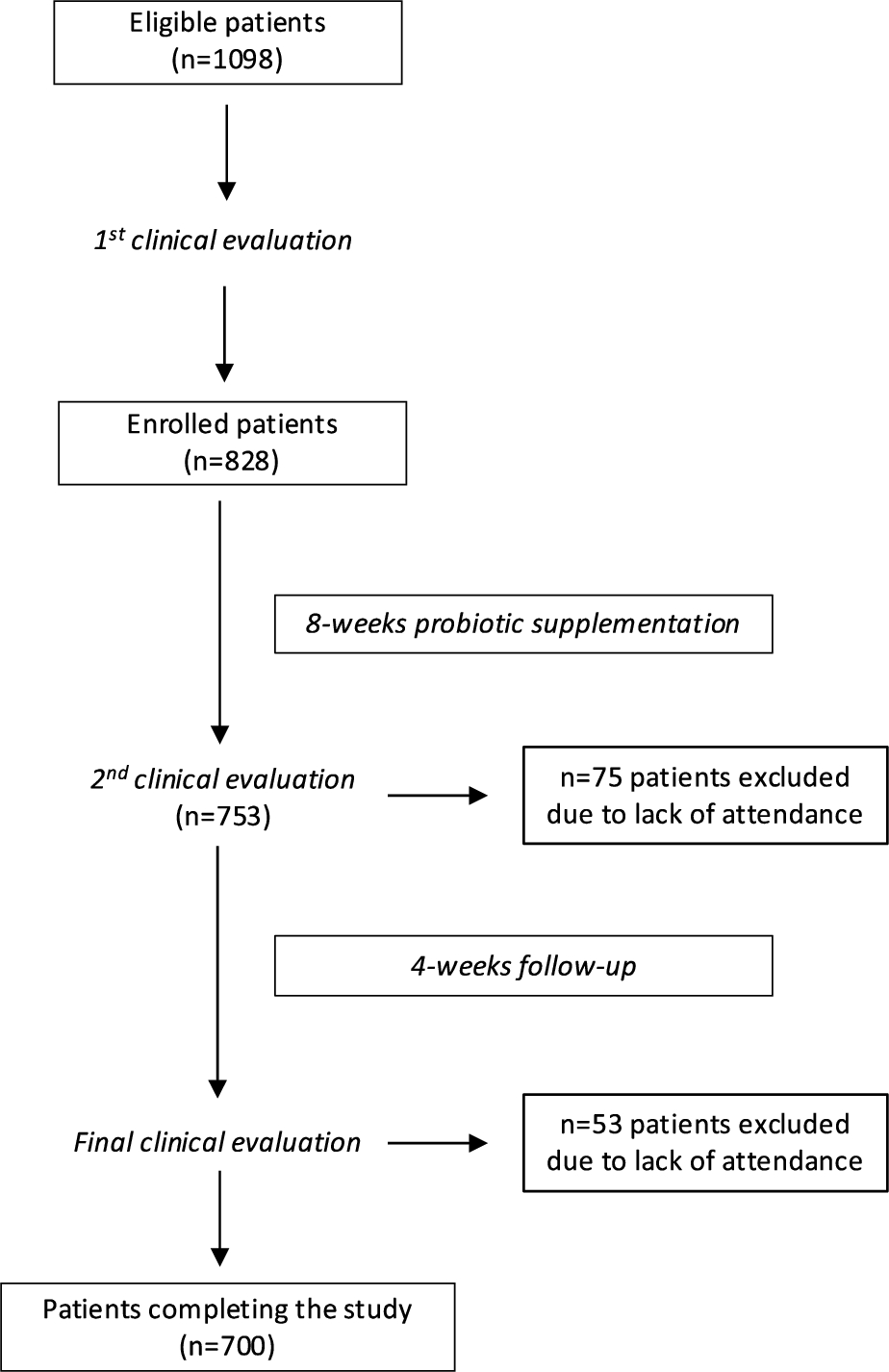
Flowchart of patients into the trial from eligibility to the end of the challenge and the timing of clinical evaluations.
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00097
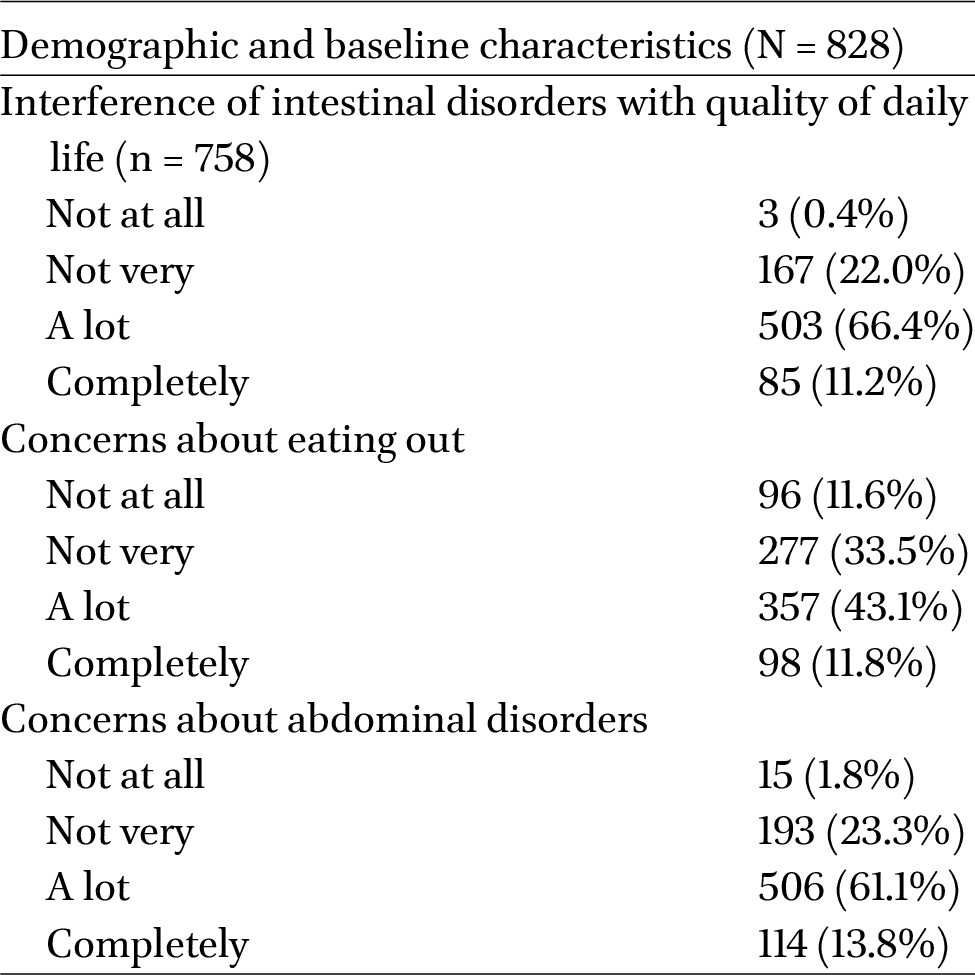
A total of 1,098 individuals were considered eligible, and 828 (75.4%) were enrolled and received the probiotic [512 F (61.9%); mean age: 46.3 ± 16.3)]. Seventy-five participants (9.1%) failed to attend the second and 53 (6.4%) the final visit (Figure 1). The body mass was categorised as usual in 60.7% of patients, overweight in 27.5%, obese in 6.6%, and underweight in 5.2%. Of the 828 patients, 428 (51.7%) had at least one pre-existing medical condition, and 295 (35.6%) had a previous surgery. The median duration of the condition was 6.9 years (95%CI: 3.4-9.6). All the subtypes of IBS were represented, and the most prevalent was mixed-IBS (IBS-M; 47.8%), followed by constipation and diarrhoea subtypes (27.9% and 24.3%, respectively). The demographic characteristics of our study population are reported in Table 1. Data on exclusion diet was available in 200 participants: 89 (44.5%) were on a lactose-free diet, 34 (17%) on a low-fibre diet, 28 (14%) were on a FODMAP diet, 27 (13.5%) were on a gluten-free diet, the remaining were on low carbohydrate (15; 7.5%), low fat (4; 2%), and nickel-free (3; 1.5%) diet. One participant identified himself as a vegetarian.
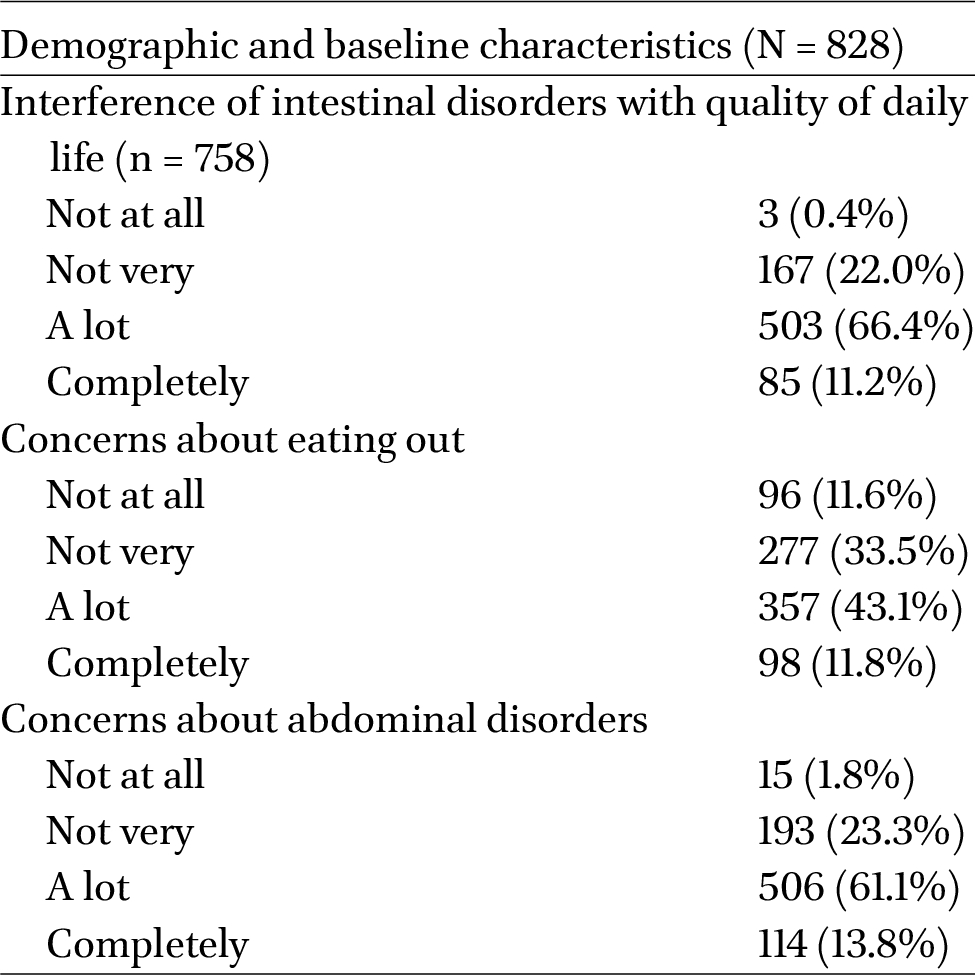
Demographic and clinical characteristics of the enrolled patients
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00097
Treatment success
In the ITT analysis, treatment success for abdominal pain was achieved in 550 participants (66.4%: CI95%: 63.1% to 69.6%) at T1 and 476 (57.5%: CI95%: 54.1% to 50.8%) at T2. Treatment success for bloating was achieved in 617 participants (74.5%; CI95%: 71.4% to 77.4%) at T1 and 512 (61.8%; CI95%: 58.5% to 65.1%) at T2. In the PP analysis, treatment success for abdominal pain was achieved 73% (CI95%: 69.7% to 76%) at T1 and 68% (CI95%: 64.4% to 71.3%) at T2. Treatment success for bloating was achieved in 81.9% (CI95%: 79% to 84.5%) at T1 and 73.1% (CI95%: 69.7% to 76.3%) at T2.
Univariate logistic regression analysis revealed no significant correlation between the achievement of the primary outcome and parameters such as patient demographics, time since diagnosis, adherence to treatment, IBS subtype, concurrent medications, comorbidities, or changes in lifestyle/eating habits during the study.
Secondary endpoints
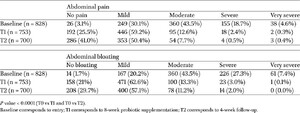
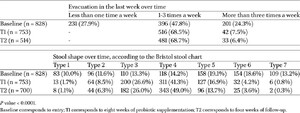
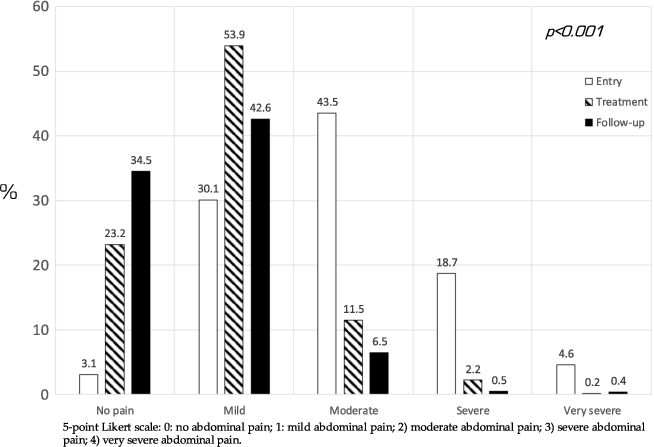
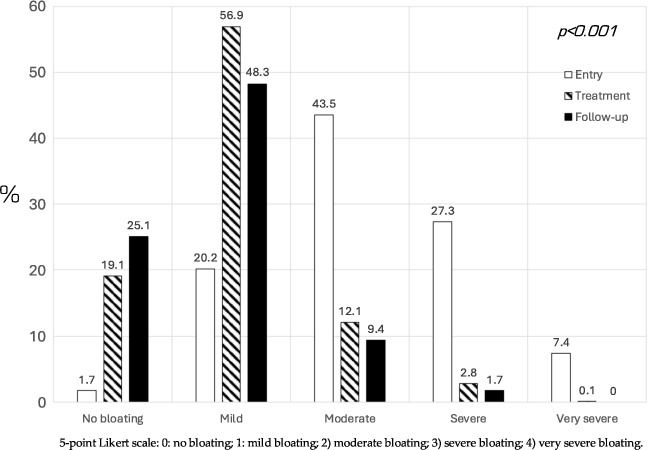
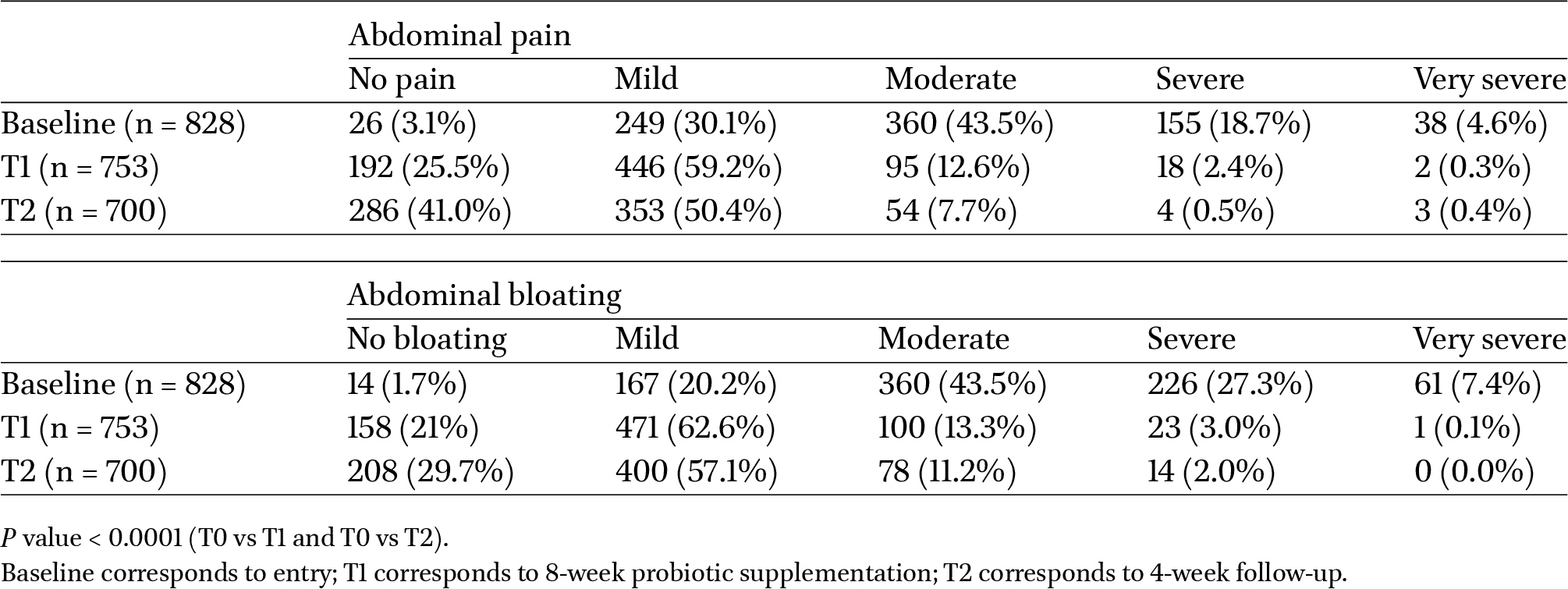
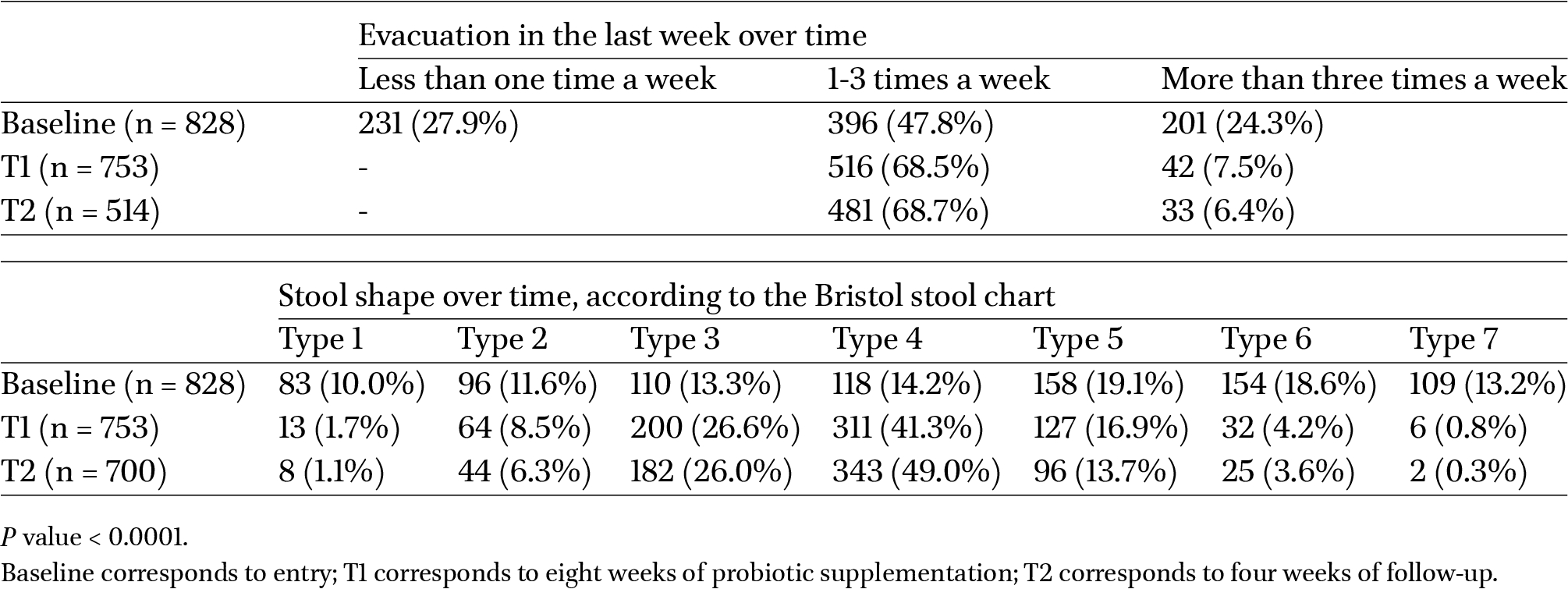
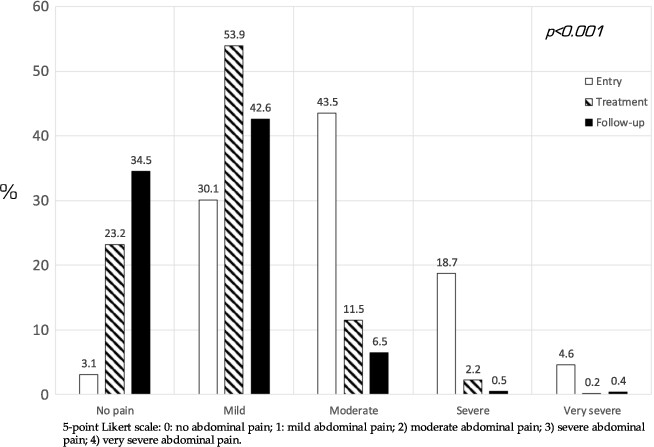
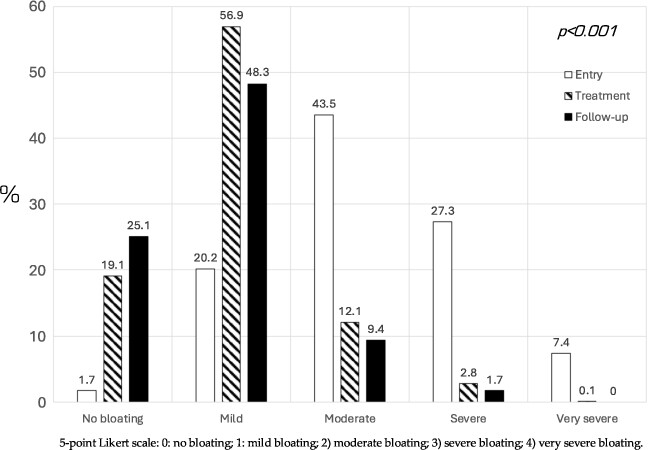
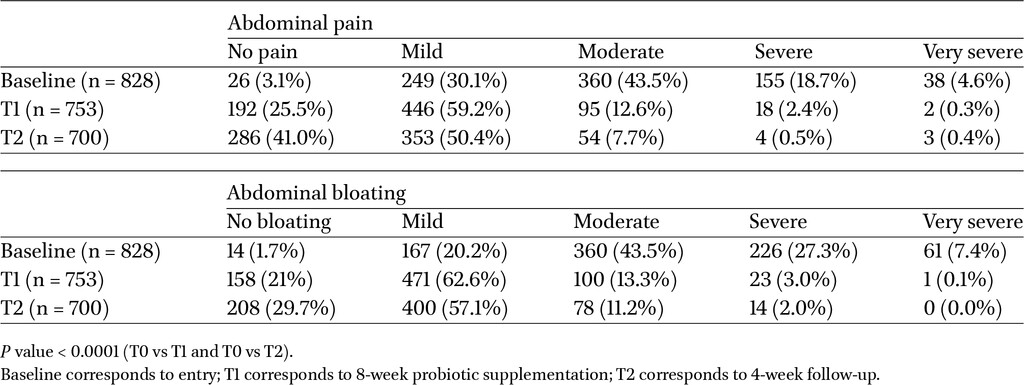
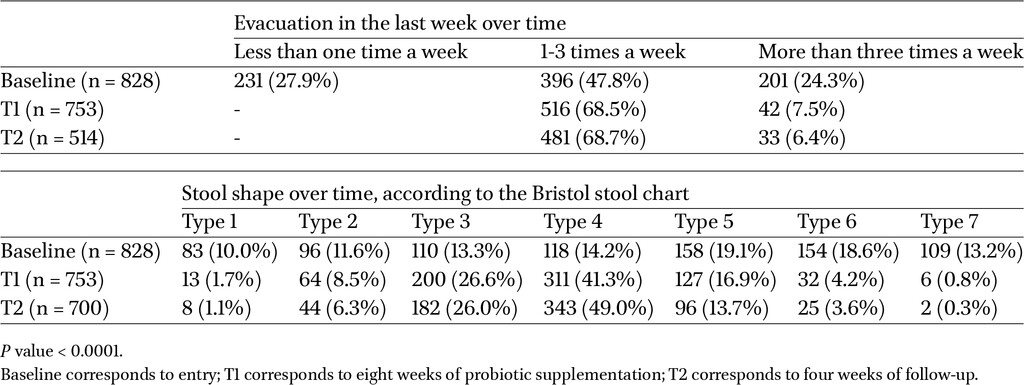
At entry, 30.1% of patients complained of mild, 43.5% of moderate, 18.7% of severe, and 4.6% of very severe abdominal pain. At the end of treatment and follow-up, the percentages changed: 53.9% and 42.6% mild, 11.5% and 6.5% moderate, 2.2% and 0.5% severe, and 0.2% and 0.4% very severe, respectively (P < 0.001). Similarly, at entry, 20.2% of patients complained of mild, 43.5% of moderate, 27.3% of severe, and 7.4% of very severe bloating. At the end of treatment and follow-up, the percentages changed as follows: 56.9% and 48.3% mild, 12.1% and 9.4% moderate, 2.8% and 1.7% severe, and 0.1% and 0% very severe, respectively (P < 0.001), (Figures 2 and 3). Table 2 shows PP analysis results. The Cochran’s Q test determined a statistically significant difference in the proportion of patients without abdominal pain or bloating over time (P < 0.001). We found no significant change in the prevalence of exclusion diets followed by patients during the duration of the study. At entry, bowel movements were in the normal range in 396 patients (47.8%), while 231 (27.9%) were constipated and 201 (24.3%) referred diarrhoea. After treatment, the number of patients with a regular bowel movement increased to 516 (62.3%; P < 0.001). A significant improvement in the typical BSC class (3-5 scores) occurred during and after the probiotic intake (T0 vs T1: P < 0.001; T0 vs T1: P < 0.001; T1 vs T2: 0.09); this improvement was consequent to a significant increase in the mean BSC score (from 2.5 ± 0.07 at T0 to 3.8 ± 0.08 at T1; P < 0.001) in patients with IBS-C and a significant decrease in the mean BSC score (from 5.8 ± 0.07 at T0 to 3.9 ± 0.08 at T1; P < 0.001) in patients with IBS-D. The variables that were analysed are reported in Table 3. During the study, the number of patients who required a diet to manage IBS decreased from 226 (27.3%) at entry to 125 (15.1%) at the end of follow-up (P < 0.001).
Frequency of abdominal pain reported by patients during all phases of the study rated according to a 5-point Likert scale from no symptoms to presence of very intense symptoms (ITT analysis).
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00097
Frequency of bloating reported by patients during all phases of the study was rated according to a 5-point Likert scale from no symptoms to presence of very intense symptoms (ITT analysis).
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00097
Progression of symptomatology (abdominal pain and bloating) during and after the probiotic treatment (PP analysis)
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00097
Progression of symptomatology (abdominal pain and bloating) during and after the probiotic treatment; P value < 0.0001 (T0 vs T1 and T0 vs T2) (PP analysis)
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00097
Impact of IBS symptoms on overall quality of life
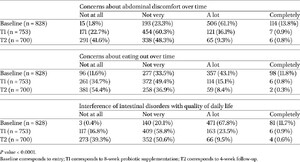
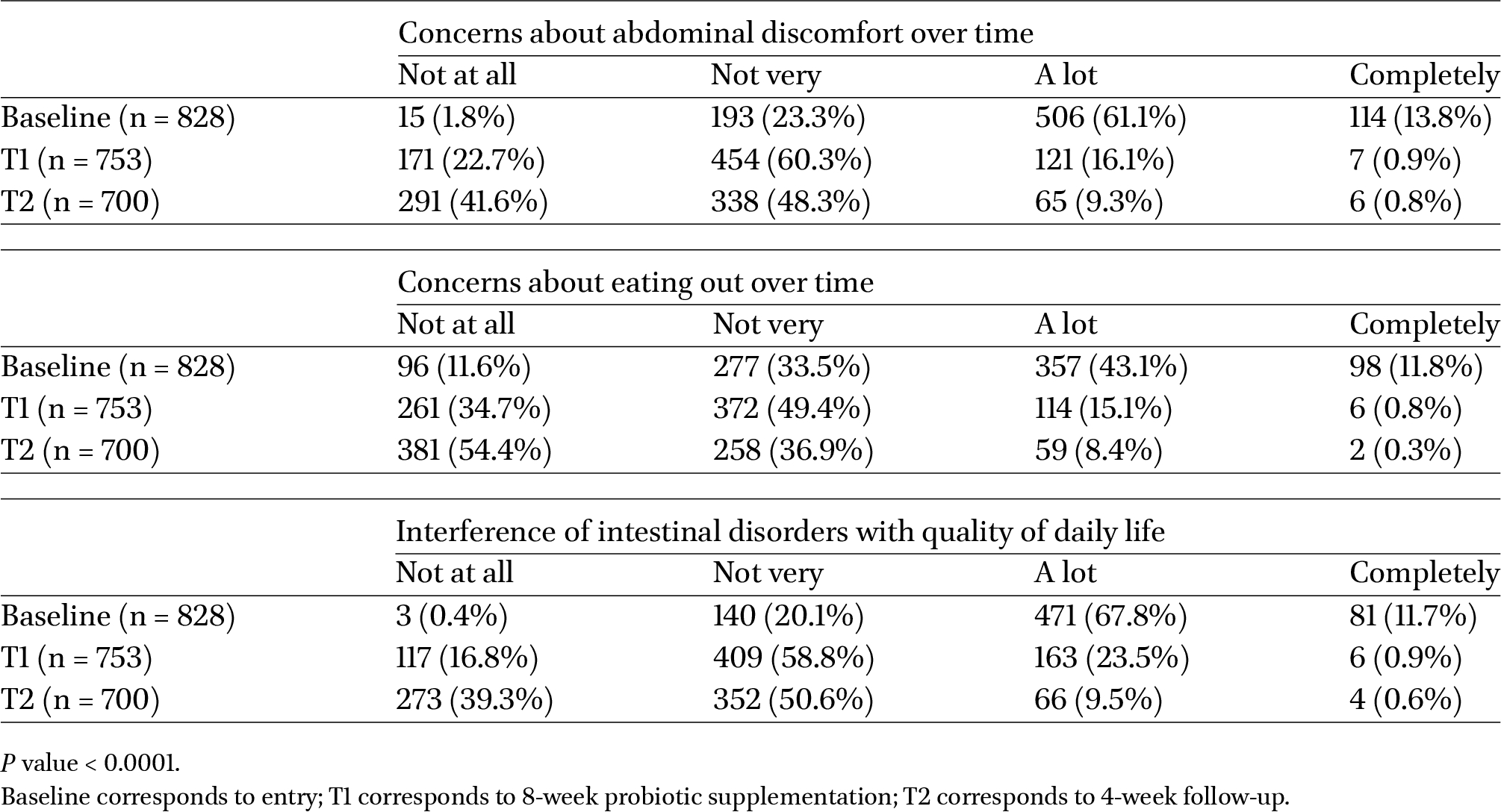
Data on concerns about ‘abdominal discomfort over time’, ‘eating out over time’, and on ‘interference of intestinal disorders with quality of daily life’ are reported in Table 4. Overall, we observed a significant improvement in all these parameters at the end of treatment and 41.6% at follow-up (P < 0.001). Complete data are reported in Table 4.
Progression of quality-of-life indicators during and after the probiotic treatment; P value < 0.0001 (T0 vs T1 and T0 vs T2) (PP analysis)
Citation: Beneficial Microbes 17, 3 (2026) ; 10.1163/18762891-bja00097
Safety
Eighty-eight per cent of patients reported satisfaction with the tested probiotics; 75.4% expressed a desire to continue consuming the supplement, and 81% indicated they were willing to recommend it to others. There were no serious adverse events, treatment-emergent adverse events, or adverse reactions during the study. All reported adverse events were mild in severity, and no participant discontinued treatment due to safety concerns. Overall, patients who completed the entire course of treatment reported no significant safety issues. At the end of the trial, 64% of the participants in the study rated the effectiveness of the study product as either ‘very good’ or ‘good.’ In comparison, 30% rated it as ‘satisfactory’.
4 Discussion and conclusion
In the present study, we describe the largest national-based open-label, observational post-marketing study on the use of a probiotic mixture on a typical population of patients with IBS. The results suggest that this probiotic mixture is effective, safe, well tolerated, and can improve patients’ social lives. Moreover, the effect extended well beyond the eight weeks of administration and persisted until the end of follow-up.
Irritable bowel syndrome is a widespread medical condition that significantly impairs the quality of life of patients and is responsible for reduced work performance. The underlying mechanisms of IBS are not entirely understood. Possible causes encompass modified gastrointestinal motility, visceral hypersensitivity, deregulation of the gut-brain axis, alterations in the composition of intestinal microbiota, and the deregulation of the immune system (Barbara et al., 2016; Fjeldheim Dale et al., 2019; Lacy et al., 2016; Van den Houte et al., 2020).
Several studies have examined the use of probiotics as therapeutic agents in IBS. A recent systematic review with meta-analysis of RCTs using ROME IV criteria has demonstrated a relevant impact of probiotics on pain and bloating; however, no indication of a particular strain or combination of strains can be suggested (Konstantis et al., 2023). We have summarised the indications and/or recommendations by Societies and Institutions for the use of probiotics in functional intestinal disorders and found that different combinations of probiotics led to notable enhancements in IBS symptoms (pain and bloating); however, no recommendation for the use of any particular strain combinations could be made rather than the use of probiotic mixtures as a collective entity (Francavilla et al., 2016).
A recent study analysed 11 trials (Fjeldheim Dale et al., 2019) and demonstrated a significant clinical improvement after using multi-strain preparations for eight weeks. In a network meta-analysis (43 RCTs), Zhang and colleagues have shown that B. coagulans was particularly effective in reducing symptom severity, L. plantarum significantly improved quality of life, and L. acidophilus provided the lowest adverse events (Zhang et al., 2022). An Italian study analysis of 104 clinical trials showed that formulations based on Lactobacillus rhamnosus and Lactobacillus acidophilus have the highest efficacy, especially for bloating and abdominal pain (Ceccherini et al., 2022). On the contrary, a Scandinavian study on 32 RCTs showed no significant difference among probiotic preparations (van der Geest et al., 2022).
IBS trials are recognised for their susceptibility to a significant placebo effect (Ford and Moayyedi, 2010). According to a meta-analysis by Patel et al., the placebo response in studies for IBS is an average of 40% (Patel et al., 2005). Our study observed a treatment success rate for abdominal pain and bloating, vastly exceeding the usual placebo value. We have studied the probiotic mixture used in the present study in 109 celiac patients suffering from IBS symptoms despite a rigorous gluten-free diet in a prospective, double-blind RCT. After six weeks, we found a significantly higher rate of treatment success, a decrease in pain on various clinical scales, and a modification of gut microbiota, with an increase in bifidobacteria that is still detectable six weeks after probiotic discontinuation only in patients receiving the probiotic (Francavilla et al., 2019). The RCT and the present investigation show that the placebo effect is aligned with what is commonly observed in IBS trials (Barberio et al., 2022).
The objective of any treatment in patients with IBS is to target the primary and/or most troubling symptoms, and this is the reason why we have focused on abdominal pain and bloating as primary outcomes. We conclude that the intake of this probiotic mixture for eight weeks had a significant impact on the symptoms in individuals with IBS. Based on these results, we thought we would expand our experience to the general population with IBS. Therefore, we have planned a real-world single-arm, open-label study since it offers insights in a setting reflecting everyday life in patients that physicians meet in routine clinical practise and are likely excluded in RCTs (e.g. because of comorbidities, non-adherence, crossover to alternative medication, and on exclusion diets). The improvement in the patient’s symptoms greatly affected the patient’s concern and attitude toward daily activities since the fear of eating ‘out of home’, the interference with daily activities, and concern for one’s health were significantly decreased during and after treatment. Although we did not directly study the quality of life with an appropriate instrument, our results clearly show improved quality of life, as demonstrated in a recent network meta-analysis enrolling 9,253 participants from 81 RCTs (Xie et al., 2023).
We observed that adverse effects with a possible causative link to supplement ingestion were extremely low and consistent with data from the literature (Francavilla et al., 2019; Lionetti et al., 2023), and we believe that the study product had an outstanding safety record. Finally, most patients rated the study product’s tolerability as ‘very good to good.’
There were several strengths in our study. First, we included individuals diagnosed based on the Rome IV criteria, and we did not impose any exclusion criteria or limitations on nutrition, lifestyle, or comorbidities. The study participants had various comorbid conditions typical of real-life patient populations. Therefore, we believe that our participants represent adult IBS patients of all ages, lifestyles, and subtypes. Second, patients were enrolled and followed by gastroenterologists who are highly experienced in managing IBS patients and familiar with the Rome IV Criteria. Physicians were well distributed in the national territory; patients represented the whole country. Finally, we evaluated several indicators simultaneously, including overall severity, total symptoms, specific symptoms, quality of life, safety, tolerability, and satisfaction.
The study was not without its shortcomings. First, the study did not include a placebo or any other comparator group that provided rigorous evidence of treatment minimising biases and controlling variables. Second, the study’s efficacy outcomes were patient-rated rather than objective biochemical indicators. Third, a post-treatment follow-up period of more than four weeks would have been more indicative of true long-term efficacy. Fourth, we assessed quality of life without using a proper questionnaire, which prevented us from gathering comprehensive data. Fifth, we did not perform stratified analyses by IBS subtype, gender, or age, as the study was not powered for such comparisons, although these factors may influence dietary habits, symptom patterns, and probiotic response. Finally, the absence of microbiological data limits the possibility of speculating that probiotics’ effect is mediated by microbiota changes, as suggested by the prolonged impact after treatment discontinuation.
The findings of this post-market single-arm, open-label study indicate that 8-week treatment with this probiotic mixture is both efficacious and well-tolerated in adult patients with IBS with varying lifestyles, comorbidities, and medications in real-world scenarios. To establish causality, rule out placebo effects, and confirm the true magnitude of benefit, well-designed randomised, placebo-controlled trials are essential and should be prioritised before drawing definitive conclusions on efficacy.
Corresponding author; e-mail: ruggiero.francavilla@uniba.it
Annicchiarico Raffaele (Taranto), Bargiggia Stefano (Milano), Battista Barbara (Cassino), Bertani Lorenzo (Pisa), Bortolan Susanna (Venezia), Bucci Antongiulio (Bari), Caldarella Maria Pia (Ortona (Ch)), Cannizzaro Renato (Pordenone), Casella Giovanni (Limbiate (Mb)), Cengia Giampaolo (Manerbio (BS)), Cicale Antonella (Napoli), Cimbalo Maria Elena (Perugia), Damiano Francesco (Napoli), D’amore Emilia (Napoli), D’angelo Francesca (Alcamo (Tp)), De Caro Vincenzo (Salerno), De Giorgio Roberto (Ferrara), Di Sarno Alessandro (Avellino), Dominijanni Domenico (Roma), Efthymakis Konstantinos (Chieti), Ferronato Antonio (Vicenza), Ferri Alessandra (Teramo), Forte Fabrizio (Matera), Forti Giacomo (Latina), Lofano Katia (Bari), Margagnoni Giovanna (Frosinone), Menasci Francesca (Roma), Milazzo Giuliano (Palermo), Morreale Gaetano (Caltanisetta), Ojetti Veronica (Roma), Panarese Alba (Taranto) Pardocchi Davide (Cagliari), Pati Antonino (Lecce), Pianese Giuseppe (Latina), Rauso Anna (Caserta), Romano Maurizio (Salerno), Sacchi Carlotta (Roma), Saggioro Alfredo (Venezia), Scaccianoce Giuseppe (Bari), Scarcella Riccardo (Sesto San Giovanni (MI)), Sediari Luca (Perugia), Sembenini Carlo (Verona), Semeraro Francesco (Taranto), Tanzilli Anna (Cassino (Fr)), Tremolaterra Fabrizio (Napoli), Vinti Maurizio (Agrigento), Zingone Fabiana (Padova).
Acknowledgements
The study was sponsored by Noos srl, Rome, Italy. The Authors offer special thanks to Dr Irene Schiavetti for the statistical support.
Authors’ contribution
Conceptualisation, methodology and formal analysis: L.D., V.D.C., R.F.; data curation, V.F.B., G.C.; original draft preparation, L.D.; G.C.; writing – review and editing, R.F., V.N.D, F.C., F.S, A.M., V.P.D.M.; supervision, G.M.; investigation, IBSdammil5 study group. All authors have read and agreed to the published version of the manuscript.
Conflict of interest
The authors declare no conflicts of interest. The funders had no role in the study’s design, in the collection, analyses, or interpretation of data, in the writing of the manuscript, or in the decision to publish the results.
Data availability
The data presented in this study are available at the request of the corresponding author for privacy reasons.
Funding
The study was unconditionally supported by Noos srl, Rome, Italy.
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Institutional review board statement
The study was conducted under the Helsinki Declaration and the ISO 14155 standard on Clinical Investigation of Medical Devices for Human Subjects – Good Clinical Practice and was approved by the institutional ethical committee (CET 46-2024; 29/12/2023).
References
Arlett, P., Kjaer, J., Broich, K. and Cooke, E., 2022. Real-world evidence in EU medicines regulation: enabling use and establishing value. Clinical Pharmacology and Therapeutics 111(1): 21-23. https://doi.org/10.1002/cpt.2479
Barbara, G., Feinle-Bisset, C., Ghoshal, U.C., Quigley, E.M., Santos, J., Vanner, S., Vergnolle, N. and Zoetendal, E.G., 2016. The intestinal microenvironment and functional gastrointestinal disorders. Gastroenterology. S0016-5085(16)00219-5. Advance online publication. https://doi.org/10.1053/j.gastro.2016.02.028
Barberio, B., Savarino, E.V., Black, C.J. and Ford, A.C., 2022. Placebo response rates in trials of licensed drugs for irritable bowel syndrome with constipation or diarrhea: meta-analysis. Clinical Gastroenterology and Hepatology 20(5): e923-e944. https://doi.org/10.1016/j.cgh.2021.08.025
Black, C.J. and Ford, A.C., 2020. Global burden of irritable bowel syndrome: trends, predictions and risk factors. Nature Reviews Gastroenterology & Hepatology 17(8): 473-486. https://doi.org/10.1038/s41575-020-0286-8
Ceccherini, C., Daniotti, S., Bearzi, C. and Re, I., 2022. Evaluating the efficacy of probiotics in IBS treatment using a systematic review of clinical trials and multi-criteria decision analysis. Nutrients 14(13): 2689. https://doi.org/10.3390/nu14132689
Chlebicz-Wójcik, A. and Śliżewska, K., 2021. Probiotics, prebiotics, and synbiotics in the irritable bowel syndrome treatment: a review. Biomolecules 11(8): 1154. https://doi.org/10.3390/biom11081154
Dale, H.F., Rasmussen, S.H., Asiller, Ö.Ö. and Lied, G.A., 2019. Probiotics in irritable bowel syndrome: an up-to-date systematic review. Nutrients 11(9): 2048. https://doi.org/10.3390/nu11092048
Drossman, D.A., Chang, L., Bellamy, N., Gallo-Torres, H.E., Lembo, A., Mearin, F., Norton, N.J. and Whorwell, P., 2011. Severity in irritable bowel syndrome: a Rome Foundation working team report. The American Journal of Gastroenterology 106(10): 1749-1760. https://doi.org/10.1038/ajg.2011.201
Drossman, D.A. and Hasler, W.L., 2016. Rome IV-functional GI disorders: disorders of gut-brain interaction. Gastroenterology 150(6): 1257-1261. https://doi.org/10.1053/j.gastro.2016.03.035
Ford, A.C. and Moayyedi, P., 2010. Meta-analysis: factors affecting placebo response rate in the irritable bowel syndrome. Alimentary Pharmacology & Therapeutics 32(2): 144-158. https://doi.org/10.1111/j.1365-2036.2010.04328.x
Francavilla, R., Cristofori, F. and Indrio, F., 2016. Indications and recommendations by societies and institutions for the use of probiotics and prebiotics in paediatric functional intestinal disorders. Journal of Pediatric Gastroenterology and Nutrition 63(Suppl 1): S36-S37. https://doi.org/10.1097/MPG.0000000000001220
Francavilla, R., Piccolo, M., Francavilla, A., Polimeno, L., Semeraro, F., Cristofori, F., Castellaneta, S., Barone, M., Indrio, F., Gobbetti, M. and De Angelis, M., 2019. Clinical and microbiological effect of a multispecies probiotic supplementation in celiac patients with persistent IBS-type symptoms: a randomized, double-blind, placebo-controlled, multicenter trial. Journal of Clinical Gastroenterology 53(3): e117-e125. https://doi.org/10.1097/MCG.0000000000001023
Guarino, A. and Canani, R.B., 2016. Probiotics in childhood diseases: from basic science to guidelines in 20 years of research and development. Journal of Pediatric Gastroenterology and Nutrition 63(Suppl 1): S1-S2. https://doi.org/10.1097/MPG.0000000000001220
Konstantis, G., Efstathiou, S., Pourzitaki, C., Kitsikidou, E., Germanidis, G. and Chourdakis, M., 2023. Efficacy and safety of probiotics in the treatment of irritable bowel syndrome: a systematic review and meta-analysis of randomised clinical trials using ROME IV criteria. Clinical Nutrition 42(5): 800-809. https://doi.org/10.1016/j.clnu.2023.03.019
Lacy, B.E., Mearin, F., Chang, L., Chey, W.D., Lembo, A.G., Simren, M. and Spiller, R., 2016. Bowel disorders. Gastroenterology 150: 1393-1407. https://doi.org/10.1053/j.gastro.2016.02.031
Lacy, B.E. and Patel, N.K., 2017. Rome criteria and a diagnostic approach to irritable bowel syndrome. Journal of Clinical Medicine 6(11): 99. https://doi.org/10.3390/jcm6110099
Lacy, B.E., Pimentel, M., Brenner, D.M., Chey, W.D., Keefer, L.A., Long, M.D. and Moshiree, B., 2021. ACG clinical guideline: management of irritable bowel syndrome. The American Journal of Gastroenterology 116(1): 17-44. https://doi.org/10.14309/ajg.0000000000001036
Leahy, A. and Epstein, O., 2001. Non-pharmacological treatments in the irritable bowel syndrome. World Journal of Gastroenterology 7(3): 313-316. https://doi.org/10.3748/wjg.v7.i3.313
Lionetti, E., Dominijanni, V., Iasevoli, M., Cimadamore, E., Acquaviva, I., Gatti, S., Monachesi, C., Catassi, G., Pino, A., Faragalli, A., Randazzo, C.L., Gesuita, R., Malamisura, B. and Catassi, C., 2023. Effects of the supplementation with a multispecies probiotic on clinical and laboratory recovery of children with newly diagnosed celiac disease: a randomized, placebo-controlled trial. Digestive and Liver Disease 55(10): 1328-1337. https://doi.org/10.1016/j.dld.2023.04.021
Miller, L.E., 2014. Study design considerations for irritable bowel syndrome clinical trials. Annals of Gastroenterology 27(4): 338-345.
Patel, S.M., Stason, W.B., Legedza, A., Ock, S.M., Kaptchuk, T.J., Conboy, L., Canenguez, K., Park, J.K., Kelly, E., Jacobson, E., Kerr, C.E. and Lembo, A.J., 2005. The placebo effect in irritable bowel syndrome trials: a meta-analysis. Neurogastroenterology and Motility 17(3): 332-340. https://doi.org/10.1111/j.1365-2982.2005.00650.x
Sperber, A.D., Bangdiwala, S.I., Drossman, D.A., Ghoshal, U.C., Simren, M., Tack, J., Whitehead, W.E., Dumitrascu, D.L., Fang, X., Fukudo, S., Kellow, J., Okeke, E., Quigley, E.M.M., Schmulson, M., Whorwell, P., Archampong, T., Adibi, P., Andresen, V., Benninga, M.A., Bonaz, B., Bor, S., Fernandez, L.B., Choi, S.C., Corazziari, E.S., Francisconi, C., Hani, A., Lazebnik, L., Lee, Y.Y., Mulak, A., Rahman, M.M., Santos, J., Setshedi, M., Syam, A.F., Vanner, S., Wong, R.K., Lopez-Colombo, A., Costa, V., Dickman, R., Kanazawa, M., Hassanzadeh Keshteli, A., Khatun, R., Maleki, I., Poitras, P., Pratap, N., Stefanyuk, O., Thomson, S., Zeevenhooven, J. and Palsson O.S., 2021. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome Foundation global study. Gastroenterology 160(1): 99-114.e3. https://doi.org/10.1053/j.gastro.2020.04.014
Van den Houte, K., Colomier, E., Schol, J., Carbone, F. and Tack, J., 2020. Recent advances in diagnosis and management of irritable bowel syndrome. Current Opinion in Psychiatry 33(5): 460-466. https://doi.org/10.1097/YCO.0000000000000628
van der Geest, A.M., Schukking, I., Brummer, R.J.M., van de Burgwal, L.H.M. and Larsen, O.F.A., 2022. Comparing probiotic and drug interventions in irritable bowel syndrome: a meta-analysis of randomised controlled trials. Beneficial Microbes 13(3): 183-194. https://doi.org/10.3920/BM2021.0123
Xie, P., Luo, M., Deng, X., Fan, J. and Xiong, L., 2023. Outcome-specific efficacy of different probiotic strains and mixtures in irritable bowel syndrome: a systematic review and network meta-analysis. Nutrients 15(17): 3856. https://doi.org/10.3390/nu15173856
Zhang, T., Zhang, C., Zhang, J., Sun, F. and Duan, L., 2022. Efficacy of probiotics for irritable bowel syndrome: a systematic review and network meta-analysis. Frontiers in Cellular and Infection Microbiology 12: 859967. https://doi.org/10.3389/fcimb.2022.859967
Appendix: Quality of Life (QOL) items used in the study
Quality of life was assessed using a customised questionnaire developed for this study to capture the specific impact of IBS symptoms on patients’ everyday lives. Participants were asked to respond to the following three items, each rated on a 4-point scale (no impact, mild impact, moderate impact, serious impact):
Concerns about eating out
‘In the past month, how much have your intestinal symptoms made you concerned about eating outside your home?’
Concerns about abdominal discomfort
‘In the past month, how much have you been concerned about your abdominal discomfort and related health issues?’
Interference of intestinal disorders with daily life
‘In the past month, how much have your intestinal symptoms interfered with your professional, social, or private daily activities?’





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}