Abstract
This double-blinded randomised controlled trial investigated whether menaquinones (MK) producing probiotics for 12 weeks improve vitamin K status, compared with placebo in 50-75 years old with at least one cardiovascular risk factor. Twenty participants were randomised to either MK-producing probiotics (n = 10) or placebo (n = 10). Plasma dephosphorylated-uncarboxylated matrix gla protein (dp-ucMGP) concentrations were the primary study outcome and determined at baseline, six and twelve weeks by a chemiluminescent InaKtif MGP assay, and analysed by linear mixed models. Secondary outcomes included serum MK-7 and phylloquinone and stool MK-4 to MK-10 and phylloquinone, assessed by linear regression. Three participants dropped out (two placebo, one intervention). Compliance was high; median 98% [IQR 96-99] and 90% [IQR 74-96] sachets used in intervention vs placebo arm. At 6 weeks, dp-ucMGP was significantly lower in the intervention group (−75.69 [95%-CI −128.37; −22.92] pmol/l), but this difference diminished by 12 weeks (−38.63 [95%-CI −94.49; 16.14] pmol/l) due to a reduction in the placebo group. Overall, the mean dp-ucMGP change over 12 weeks favoured the intervention (−59.89 [95%-CI −110.7; −9.187] pmol/l). Statistically significant differences in secondary outcomes included higher serum MK-7, and faecal MK-6 and MK-7 concentrations in the probiotic vs placebo arm (e.g. 4.41 [95%-CI 2.17; 6.65] μg/L for serum MK-7). No other secondary outcomes differed significantly. MK producing probiotics may enhance vitamin K status in older adults at elevated cardiovascular risk. Larger, longer-term studies are needed to assess functional outcomes.
The Netherlands Trial Register: NTR7505, 27-09-2018.
1 Introduction
Vitamin K plays a crucial role in human health as a cofactor in the carboxylation (activation) of the enzyme gamma-glutamyl carboxylase, which serves to catalyse the gamma-glutamyl carboxylation of glutamic acid residues (Gla) in so-called vitamin K-dependent proteins (Furie et al., 1999). These proteins not only include the hepatic coagulation factors II (prothrombin), VII, IX, and X, but also extra-hepatic proteins such as matrix gla protein (MGP), an important inhibitor of vascular calcification. Through these vitamin K-dependent proteins, vitamin K plays a well-established role in coagulation, vascular calcification and bone metabolism (Beulens et al., 2013).
Vitamin K is present in two forms in our diet: (1) plant-derived phylloquinone (vitamin K1), predominantly found in green leafy vegetables (Bolton-Smith et al., 2000), and (2) bacterial-derived menaquinones (MKs, vitamin K2), e.g. derived from cheese, sauerkraut, curd and natto (a traditional Japanese food composed of fermented soya beans) (Beulens et al., 2013; Schurgers and Vermeer, 2000; Van Ballegooijen and Beulens, 2017). In Western diets, vitamin K intake comes mainly from phylloquinone (90%), while MKs account only for 10% (Beulens et al., 2013). However, absorption of phylloquinone from vegetables is limited with only 10-20% bioavailability (Beulens et al., 2013). Older adults often have reduced vitamin K intake due to diminished appetite, reduced dietary diversity or dietary restrictions, putting them at risk of vitamin K deficiency, which may negatively impact health (Booth et al., 2003; Van Ballegooijen et al., 2018).
A potential strategy to improve vitamin K status in older adults is supplementation with probiotics. Probiotics are live micro-organisms that confer health benefits on the host when administered in adequate amounts, with some strains showing documented effects on gastrointestinal health, immune modulation and cardiometabolic risk factors (Salminen et al., 2021; Valdes et al., 2018). Probiotics are already widely used by older adults, particularly to support digestive health and prevent antibiotic associated side effects, making them a familiar and acceptable intervention in this population (Östlund-Lagerström et al., 2016). This existing use further supports their potential as a practical vehicle for MK delivery. Certain probiotic strains have demonstrated the ability to synthesise MKs in vitro and may thereby contribute to vitamin K status (Chollet et al., 2017; Mazhar et al., 2022; Tan et al., 2021). However, the extent to which intestinal production can cover vitamin K requirements is debated since the route of absorption remains unclear and production may occur throughout the gut (Beulens et al., 2013; Kang et al., 2022; Suttie, 1995). The presence of MK-producing microbiota in the gut suggests the potential for sustained endogenous synthesis of MKs, which may contribute to the host’s vitamin K status alongside dietary intake. In addition, unlike traditional vitamin K supplements, which primarily focus on MK-4 and MK7, probiotics may produce a broader range of MKs. This diversity may be advantageous given the potential for different MK species to vary in bioavailability, tissue distribution and half-life, though the functional relevance of these differences requires further investigation (Walther et al., 2013). Although the effects of direct vitamin K2 supplementation on circulating MKs and dp-ucMGP are well established, it remains unknown whether MK-producing probiotics can similarly modulate vitamin K status in humans. To date, no randomised controlled trials have evaluated whether bacterially derived menaquinones from probiotic strains are absorbed and can influence extra-hepatic vitamin K-dependent proteins. This represents an important knowledge gap, given the increasing availability of MK-producing probiotics and their potential to serve as an alternative delivery route distinct from traditional supplementation. Given that certain probiotic strains are widely available and regarded as safe by the European Food Safety Authority (EFSA) (EFSA Panel on Biological Hazards et al., 2024) and that probiotics are already commonly prescribed in nursing homes to increase intestinal health and reduce obstipation, they may present an accessible and promising approach for adults, particularly those with subclinical vitamin K deficiency, when strains with MK producing capacity are selected.
This study aimed to investigate whether a 12-week supplementation with MK-producing probiotics versus placebo could increase vitamin K status in middle-aged adults between 50-75 years at elevated cardiovascular disease risk. Vitamin K status was measured as primary outcome and evaluated through assessment of dephosphorylated-uncarboxylated MGP (dp-ucMGP; inactive MGP), which is proposed as a biomarker for vitamin K status with high concentrations indicating low vitamin K status (Cranenburg et al., 2010; Dalmeijer et al., 2012). Secondary outcomes included serum MK-7 and phylloquinone concentration and stool MK-4 to MK-10 and phylloquinone concentration. We hypothesised that probiotics with MK producing properties can improve vitamin K status.
2 Materials and methods
Study design
This double-blind, randomised, controlled trial (RCT), assessed the effect of probiotics with MK producing bacteria versus placebo on vitamin K status after 12 weeks amongst people aged 50-75 years at elevated risk of cardiovascular disease. This study population was chosen, because a low vitamin K status and intake have been associated with increased risks of cardiovascular disease (Lees et al., 2019). Participants were 1:1 allocated to either the intervention arm (probiotics) or the placebo arm. Participants were eligible for participation in case they had at least one of the following cardiovascular risk factors: high blood pressure (>90/140 mmHg) or use of blood pressure lowering medication; increased non-fasting glucose levels (≥7.8 and <11.1 mmol); family history of cardiovascular disease; elevated cholesterol levels (>6.5 mmol/l) or use of statins; smoking or elevated glomerular filtration rates. Participants with a diagnosis of diabetes; bowel disorders; a body mass index (BMI) below 20 or higher than 39 kg/m2; or who consumed more than three alcoholic beverages a day were excluded. Participants were not allowed to use vitamin K or probiotic supplements, vitamin K antagonists or dietary products high in vitamin K content (natto or goose liver) during, or in the two weeks before start of the study. Potential participants who used antibiotics in the three months before the study were excluded as well. Participants visited the Research Centre in Hoorn (the Netherlands) four times: once for a screening visit, once for a baseline visit and twice (six and twelve weeks after the baseline visit) for follow-up visits. This study was conducted according to the principles of the Declaration of Helsinki (Fortaleza, Brazil October 2013) and in accordance with the Medical Research Involving Human Subjects Act (WMO). The study protocol was approved by the Medical Ethical Committee from VUmc, registration number NL71758.029.19. The trial was registered before commence of the study at the Netherlands Trial Register NTR7505, and can be accessed through the Netherlands Trial Register (CCMO): Het effect van probiotica op vitamine K status | Onderzoek met mensen. All participants provided written informed consent. This manuscript was written in line with the Consolidated Standards of Reporting Trials Statement (CONSORT) 2010 guidelines (Schulz et al., 2010).
Recruitment
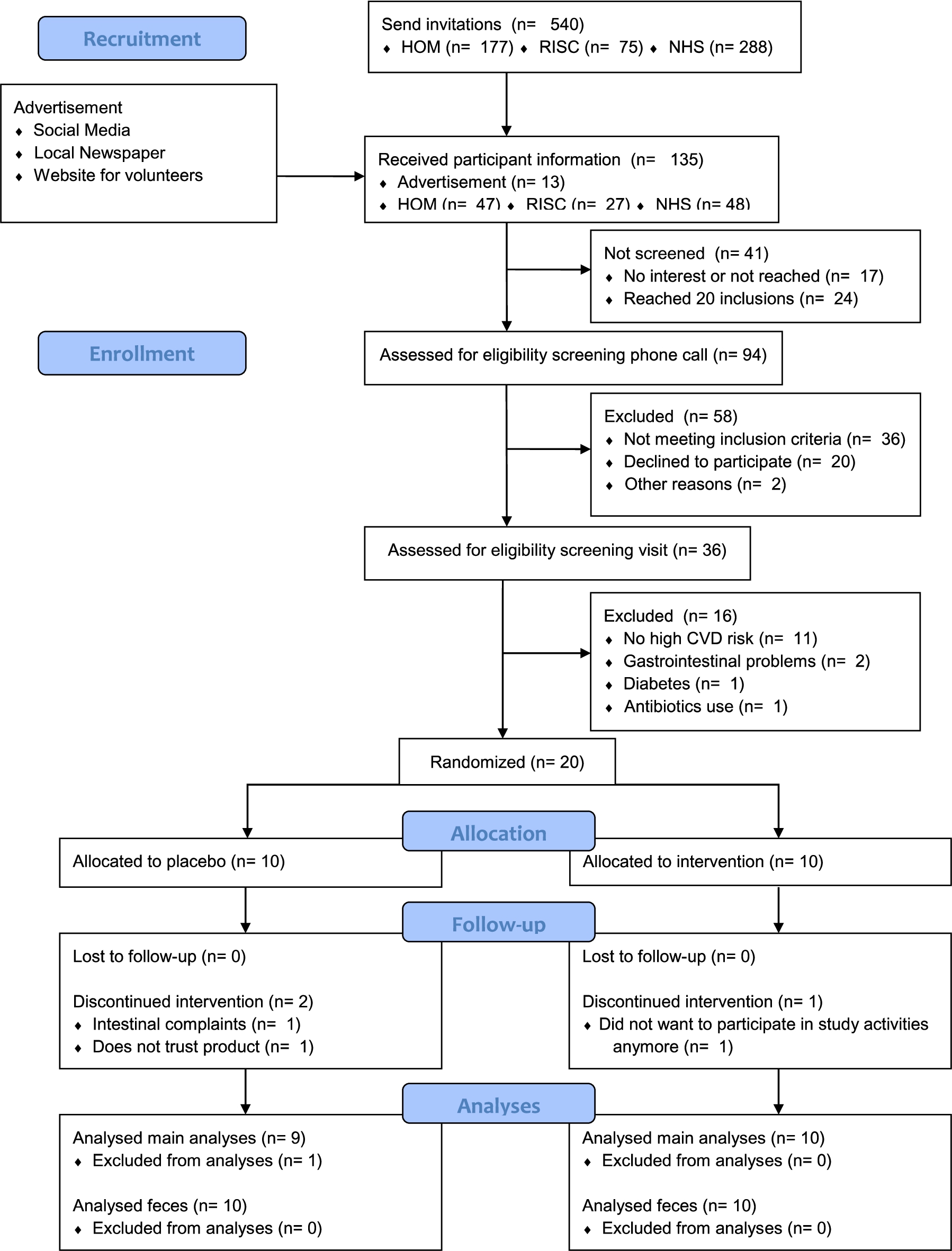
Participants from previous research who provided consent for future studies were invited to participate in this study. In addition, we used advertisements on social media, in a local newspaper and on a website for volunteers to recruit participants. Recruitment proved difficult, hence we broadened the age range of eligible participants from 50-70 years to 50-75 years. No other changes were made to the original study protocol. A total of 540 people who participated in previous studies were invited, and the response rate was 22.6% (SK; Figure 1). The advertisements resulted in 13 persons who expressed their interest to participate in the study. Eligibility was first assessed during a screening phone call (n = 94), during which 58 people did not meet the inclusion criteria and 20 were not willing to participate, two did not attend a screening visit for different reasons. A screening visit followed for 36 people, of whom 11 were not eligible since they were not at high cardiovascular risk, two had bowel disorders, one had diabetes and one used antibiotics. Finally, 20 participants were randomised.

CONSORT flow diagram of study participants.
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00117
Investigational product
The investigational product was manufactured and supplied by Winclove Probiotics b.v. (Amsterdam, the Netherlands) and consisted of a daily sachet of four-gram freeze-dried probiotics. Each gram of product contained 2 × 1010 cfu, with four bacterial species which were selected for their capacities to produce higher concentrations of MK-7 to MK-10 namely: Lactococcus lactis W58, Bacillus subtilis W201, Bacillus coagulans W64 and Propionibacterium freudenreichii W200 (in a ratio of 1:1:15:25) (Bøe and Holo, 2020; Furuichi et al., 2006; Huang et al., 2024; Liu et al., 2019; Rowland et al., 1995; Yang et al., 2019; Zhang et al., 2025). Every single probiotic strain was measured for its MK concentration, before mixing all strains in one probiotic blend. Based on the MK amount that each probiotic strain contained in its cell, the total amount of MKs was set to 180 μg/dosage (4 g). Among the isoforms, MK-7, MK-9 and MK-10 were present at the highest concentrations, while the rest (MK4, MK5, MK6, MK8) were present in much lower concentrations. In other words, the investigational product contains 180 μg of menaquinones, of which menaquinones with longer side chains are present in high concentrations, contrary to menaquinones with shorter side chains. This said, we assume that absorption rates may be high due to the high concentration of long side chain-menaquinones included in the product. Since the investigational product is a commercial product and IP rights are linked to it, the exact composition cannot be revealed. This way of producing the probiotic blend allowed to be certain that every sachet contained the same amount of MKs. The placebo was indistinguishable in colour, smell and taste from the probiotic supplement, but without live bacteria. The other ingredients in both the investigational product and placebo were cornstarch and maltodextrins. Participants of both groups were asked to mix the content of the sachet with a cup of yoghurt or custard and to consume one sachet of the assigned product per day.
Study visits
The screening visits took place between 22-11-2021 and 18-01-2022, while the study visits were conducted between 9-12-2021 and 11-05-2022 (SK). The fact that recruitment and screening were conducted on a continuous basis, allowed us to start the baseline visit and intervention period for the first eligible participants, while screening of later participants was still ongoing. Participants were asked to remain in the fasted state from 22:00 h the night before the study visits until the study visit itself. During the screening visit, questions were answered, informed consent was signed and eligibility criteria were assessed. Medical history and vitamin K intake were checked using questionnaires. The dietary questionnaire included products rich in vitamin K content such as green leafy vegetables, cheese, soft curd cheese and natto. Blood pressure was measured by a Welch Allyn NIBP 3400 sphygmomanometer (Navan, Ireland). Weight and height were measured while participants were barefoot and wearing light clothes. BMI was calculated by dividing kilograms of weight by the square of height in meters. Non-fasted blood samples were collected with a finger prick, after which glucose was directly measured with the Roche (Basel, Switzerland) Accu-Check Aviva point of care test. Cholesterol levels were determined with an enzymatic colorimetric test via the Roche-Hitachi Cobas C systems, by the Amsterdam UMC, VUmc clinical laboratory. In case of eligibility, participants were randomised and a baseline visit followed. Baseline measurements were taken and instructions regarding the use of the products were given. After six and twelve weeks, follow-up visits followed. During each of the study visits, blood pressure, BMI, and intake of vitamin K rich foods in the past two weeks were registered. Fasting serum and plasma EDTA were collected and stored at −80 °C. Additionally, participants were asked to collect stool samples at home preferentially the day before the study visit and store the samples in their freezer. Samples were taken to the test centre by the participant, and then stored at −80 °C until further processing. Participants were asked to keep both the used and unused sachets and bring them back to the research centre during the follow-up visits. Compliance was assessed by counting both the opened and unopened sachets. Participants were also asked about any adverse events or complaints during the follow-up visit. Participants filled in a questionnaire at each study visit about the frequency of consumption of vitamin K rich products including different green vegetables, fruits, dairy products, meat products and natto.
Randomisation and blinding
Both the study investigators and the participants were blinded for the allocation of study arms until the database was locked and data was analysed. An employee from Winclove Probiotics b.v. who was not involved in the study and were blinded to any of the participants information, block randomised the participants in blocks of four to ensure balanced participant characteristics in both intervention and placebo groups. Allocation was determined using computer generated random numbers. All study products were sequentially numbered, and the coded study products were sent to the research centre. The randomisation code was stored in a sealed envelope until the end of the study, and kept save by the principal investigator (JB). This allowed for the possibility of revealing treatment allocation code in case of medical emergencies, however this was not needed and the envelope remained sealed until the database was locked (MM). No patient information was shared with Winclove Probiotics b.v. neither before, during nor after the randomisation process.
Laboratory measurements
Metabolite measurements took place at Coagulation Profile, Maastricht University. Circulating dp-ucMGP concentrations were determined in EDTA plasma using the IVD CE marked chemiluminescent InaKtif MGP assay on the IDS-iSYS system (IDK, Boldon, UK). Samples of 50 μl were incubated with magnetic particles covered in murine monoclonal dpMGP antibody, assay buffer and an acridinium labelled murine monoclonal ucMGP antibody. The magnetic particles were captured using a magnet and subsequently a washing step was performed to remove unbound analyte. Trigger reagents were added and the resulting light emitted by the acridinium label was directly proportional to the dp-ucMGP concentration in the sample. The within-run and total precision of this assay were 0.8-6.2% and 3.0-8.2%, respectively. The assay measuring range is between 300-12,000 pmol/l and was found to be linear up to 11,651 pmol/l. dp-ucMGP values below 300 pmol/l were considered to be in the normal healthy range. Assays were performed in a single run by Coagulation Profile BV, Maastricht, the Netherlands.
Phylloquinone and MK-7 were determined in serum; 0.5 ml of serum was diluted 1:1 with dH2O and then mixed with 2 ml of ethanol containing 2 ng of the internal standard 2’,3’-dihydro-phylloquinone. The mixture was homogenised and extraction of K vitamins was done using hexane. After prepurification over silica Sep-Pak cartridges, vitamin K was analysed by HPLC using a C18 reversed phase column and fluorometric detection after post-column zinc reduction as described previously (Schurgers and Vermeer, 2000). Phylloquinone and MKs were recorded in the same run. The interday variation was 6-8%. Faeces were mixed with water, ethanol and internal standard. The mixture was heated at 70 °C for 30 min. Afterwards, samples were cooled down and hexane was added. Samples were centrifuged and the upper layer containing vitamin K was evaporated under a stream of nitrogen. Vitamin K concentrations in faeces samples were measured by high performance liquid chromatography (HPLC) and fluorescence detection after on-line, post-column zinc reduction of the effluent, which converted the quinone forms of vitamin K compounds to their fluorescent quinol forms (Schurgers et al., 2007). The lower limit of quantification for this assay was typically 0.05 μg/l (both serum and faeces). Phylloquinone was obtained from Sigma (St. Louis, MO, USA). The MK-4 through MK-10 and 2,3-dihydrophylloquinone were kind gifts from Hoffmann-La Roche (Basel, Switzerland). Silica Sep-Pak cartridges were purchased from Millipore (Milford, MA, USA). All other chemicals used were of the highest analytical grade. All analyses were performed according to validated laboratory protocols. Serum and faecal samples were analysed in a limited number of analytical batches, each including calibration curves, internal standards and quality control samples to monitor assay performance and drift. Sample order within each batch was randomised to minimise potential batch effects. All biological samples were stored at −80 °C and were thawed only once prior to analysis to prevent degradation.
Although urine metabolites were listed as exploratory outcomes in the trial registration, these were not analysed due to delays in the development of the required analytical method by the collaborating laboratory.
Sample size calculation
No previous studies have investigated the effect of probiotics with vitamin K producing bacteria to increase vitamin K status. Therefore, our sample size calculation was based on studies with similar dosages of MK-7. With a dose of approximately 180 μg MK-7 reductions of 17-40% in dp-ucMGP were observed (Caluwe et al., 2014; Dalmeijer et al., 2012; Theuwissen et al., 2012; Westenfeld et al., 2012). Our product contains probiotics that are expected to produce approximately 180 μg of various MKs in the intestine after ingestion, based on prior characterisation of the strains. Therefore we expect an effect size of −30% dp-ucMGP. The average effect size was 120 pmol/l in healthy adults with a standard deviation (SD) of 110 pmol/l (Dalmeijer et al., 2012). Based on an SD of 110 pmol/l, we calculated the SD of the difference between baseline and follow-up using the formula
Baseline characteristics of 20 people for the total population and for intervention (probiotics) and control (placebo) group, separately1
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00117
Statistical analyses
Baseline characteristics of the participants are shown as mean and SD, median and interquartile range or frequency and percentage, stratified by study arm. A linear mixed model regression with a random intercept for participant ID was used to assess the difference in change in dp-ucMGP levels over 12 weeks between the intervention and control arm. The analyses were adjusted for baseline dp-ucMGP levels to minimise the chance that a pre-existing imbalance between study arms, despite randomisation of participants, influenced the study findings. Additionally, an interaction term for timepoints was added to the model, enabling assessment of the difference in change in dp-ucMGP levels after 6 an 12 weeks, separately. Secondary outcomes (MK-7 and phylloquinone in serum; MK-4 to MK-10 and phylloquinone in stool) were assessed with linear regression, adjusted for baseline metabolite concentrations. In order to meet the normality of the residuals assumption for linear regression analysis, MK-7 concentrations in faeces were log-transformed and presented as back transformed regression coefficients, representing ratios of geometric mean. A linear mixed model regression analysis, which can handle missing time points, was used for the primary outcome (dp-ucMGP). For one participant in which baseline blood measurements were missing, data were excluded in all the plasma or serum based statistical analyses. Three participants dropped out between the six and twelve weeks visit. In these participants, the last observation at six weeks was carried forward in the analyses of the secondary outcomes which were evaluated by means of linear regression analyses. Although multiple imputation is generally preferred for handling missing data, our study’s small sample size precluded reliable implementation. We therefore used Last Observation Carried Forward as a pragmatic alternative, while recognising its limitations and potential for bias. We imputed half the limit of detection metabolite values below the detection limit. Sensitivity analyses were performed by only including participants in the analyses with a compliance higher than 80% based on sachet count. All analyses and data visualisation were conducted in R Studio version 4.0.3 (R Core Team, 2021). Statistical significance was set at a two-sided
3 Results
The mean age of the participants in the intervention arm and placebo arm was 62.8 (SD 4.49) and 66.6 (SD 3.81) years, respectively, (Table 1). More women than men participated in the trial, 60% in the intervention and 70% in the placebo arm. Dp-ucMGP concentrations were 616 (SD 98) pmol/l in the probiotics vs 643 (SD 122) in the placebo group. None of the participants was lost to follow-up at six weeks, but three participants were lost to follow-up after twelve weeks. Of these, two were assigned to the placebo and one to the intervention arm. The participants in the placebo arm reported intestinal complaints, and to not trust the product, while the participant lost to follow-up in the intervention arm did not want to participate in study activities anymore. Overall, compliance was high, and somewhat higher in the intervention compared to the placebo arm (median of 98% [IQR 96-99] and 90% [IQR 74-96] in the intervention vs the placebo arm). Seven participants in the placebo and nine participants in the intervention arm reached a compliance of at least 80%. Frequency of consumption of vitamin k rich products did not differ between study arms and over time (Supplementary Table S1).
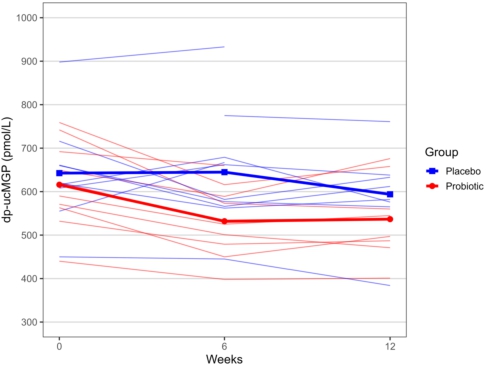
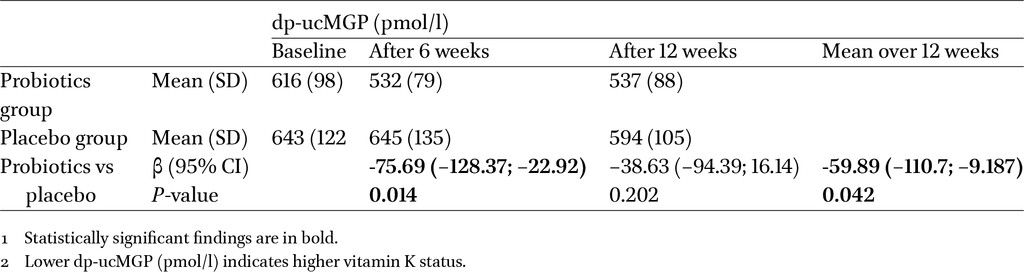
Change in mean (SD) dp-ucMGP (pmol/l) concentrations over 6 and 12 weeks in the probiotics group vs the placebo group, missing data were omitted.
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00117
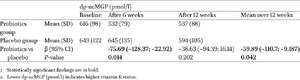
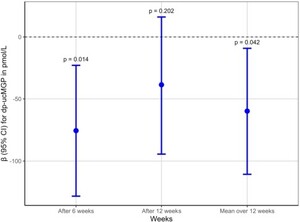
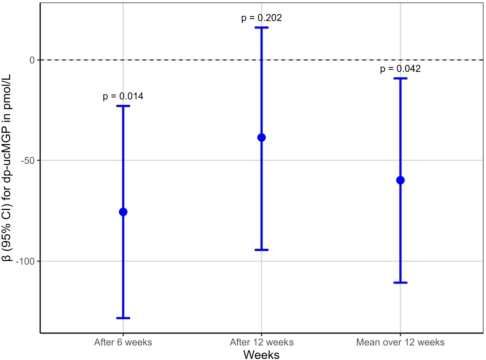
Primary outcome: change in dp-ucMGP (pmol/l) over 6 and 12 weeks in the probiotics group (n = 10) vs the placebo group (n = 9)1,2
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00117
Primary outcome: change in dp-ucMGP (pmol/l) over 6 and 12 weeks in the probiotics group (n = 10) vs the placebo group (n = 9).
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00117
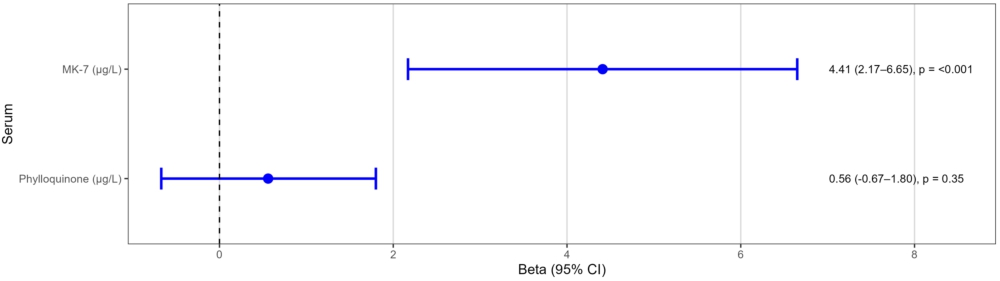
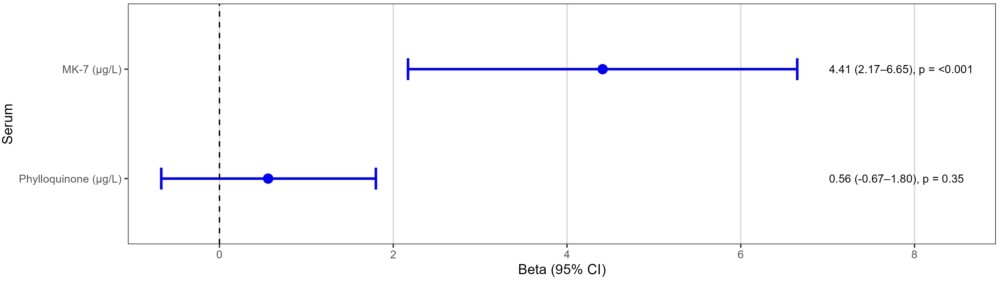
After six weeks of probiotics, dp-ucMGP concentrations changed by −75.69 (95%-CI −128.37; −22.92) in the intervention vs placebo group. Figure 2 shows that the reduction in dp-ucMGP concentrations the intervention group remained stable from week six to twelve. In the placebo group, dp-ucMGP concentrations remained stable at 6 weeks compared to baseline concentrations, but decreased somewhat after 12 weeks. The mean decrease in primary outcome dp-ucMGP over the entire 12 week period was larger in the intervention than in the placebo arm, with a difference in change between groups of −59.89 (95%-CI −110.7; -9.187) pmol/l (Table 2 and Figure 3). However, the difference in dp-ucMGP decrease between both groups was larger after six than after twelve weeks due to a decrease in the placebo group between six and twelve weeks (−75.69 [95%-CI −128.4; −22.92] vs −38.63 [95% CI −94.30; 16.14]), and the difference was no longer statistically significant at twelve weeks. Secondary outcomes were assessed after twelve weeks. For serum vitamin K concentrations, no statistical difference in change in phylloquinone was observed with a 0.56 [95%CI −0.67; 1.80] μg/l increase in the intervention vs placebo arm (Figure 4). A statistically significant increase in MK-7 was observed, with a 4.41 [95% CI 2.17; 6.65] μg/l increase in the intervention arm compared to the placebo arm. This is in line with the findings in faeces (Figure 5); no statistical differences in phylloquinone concentrations were observed, while MK-7 was 3.68 [2.20; 6.14] times higher in the intervention vs placebo arm. A significant increase was also observed for faecal MK-6 concentrations (0.30 [95% CI 0.07; 0.54] μg/g). None of the other MKs showed statistically significant differences between the probiotics and placebo arms after 12 weeks. Sensitivity analyses excluding participants with a low compliance (<80%; n = 3) did not change our findings (Supplementary Table S3 and S4). A total of six participants in the probiotics versus three in the placebo group reported changes in bowel habits. Reported symptoms included harder stool or constipation (n = 4 in the probiotics group; n = 1 in the placebo group), softer stool or diarrhoea (n = 3 vs n = 2), and increased urgency or pain during bowel movements (n = 1 vs n-1). Abdominal discomfort (e.g. flatulence, bloating, or rumbling intestines) was reported by two participants in the probiotics groups and three in the placebo group. No other side effects were reported. No substantial differences between study arms in consumption of vitamin K rich products was reported during follow-up.
Secondary outcomes: change in phylloquinone and menaquinones concentration in serum over 12 weeks in the probiotics group (n = 9) vs the placebo group (n = 10). n = 9 for the placebo group due to one missing blood sample at baseline.
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00117
Secondary outcomes: change in phylloquinone and menaquinones concentration in faeces over 12 weeks in the probiotics group (n = 10) vs the placebo group (n = 10).
Citation: Beneficial Microbes 2026; 10.1163/18762891-bja00117
4 Discussion and conclusions
This study is the first to investigate the effect of MK producing probiotics supplements on vitamin K status in people at elevated cardiovascular risk. This study showed that 12 weeks of probiotics supplementation reduced plasma dp-ucMGP by approximately 10 to 15% compared with placebo, reflecting an improved vitamin K status. However, a greater reduction in dp-ucMGP was observed at 6 weeks in the intervention group, but this difference attenuated and was no longer statistically significant by 12 weeks due to a reduction in the placebo group. In line with these findings, serum MK-7 and faeces MK-6 and MK-7 concentrations also increased after probiotics supplementation compared with placebo. However, No statistical differences were observed for any of the other considered secondary outcomes, nor for dp-ucMGP after 12 weeks.
This study had several strengths including its randomised, placebo-controlled, double-blind design, high compliance and inclusion of a relevant study population of participants at elevated cardiovascular risk. Nevertheless, several limitations need to be addressed. Although the study was sufficiently powered for the primary outcome, this study had a relatively small sample size. This may have led to both false-positive and false-negative findings, and especially precluded us to detect differences with weak effect sizes. In addition, the trial is not sufficiently powered to study potential effect modification by certain characteristics such as sex or age. We used a combination of different probiotic strains that produce different MKs in different amounts. We can therefore not specifically attribute the observed effects to specific strains or MKs. A further consideration is that vitamin K status was assessed using dp-ucMGP as the only interpretable vitamin K-dependent protein biomarker. Although total MGP may provide additional mechanistic insight, a validated assay for total circulating MGP is not currently available, and dp-ucMGP is the only established method. PIVKA-II concentrations were near the assay’s lower detection limit, and therefore did not contribute interpretable information. Another limitation is the absence of microbiome profiling. We did not assess baseline abundance of MK-producing bacteria, changes in microbial composition or persistence of the supplemented strains. Although increases in faecal MK-6 and MK-7 provide indirect evidence of microbial MK production, these changes cannot be directly linked to specific strains or shifts in microbial abundance. Future studies should therefore include metagenomic sequencing and strain-specific analyses to determine colonisation, microbiome dynamics and the long-term contribution of probiotic-derived MKs to host vitamin K status. Finally, although small differences in the reported frequency of vitamin K-rich food intake were observed between groups at weeks 6 and 12, these differences were minor in comparison to the dosage of the supplements. Moreover, the substantial increases in serum and faecal MK-7 observed in the intervention group are unlikely to be explained by diet alone, as these isoforms are not typically consumed in high amounts in a Western diet (Beulens et al., 2013). Therefore, diet may represent a minor residual confounder but is unlikely to account for the observed differences.
A key finding of this study is that the between-group difference in vitamin K status, as measured by dp-ucMGP, was evident at 6 weeks, but not sustained at 12 weeks. The intervention group exhibited a marked reduction in dp-ucMGP concentrations between baseline and 6 weeks, with levels stabilising thereafter. In contrast, the placebo group did not have a reduction in dp-ucMGP concentrations between 0 and 6 weeks, but showed a delayed and smaller reduction in dp-ucMGP between weeks 6 and 12, thereby diminishing the between-group difference at the end of the study. The reason for this decline in the placebo group is unclear, but may reflect random variation, changes in dietary vitamin K intake, regression to the mean or other unmeasured factors. Given the small sample size, caution is warranted in interpreting these patterns. Nevertheless, the overall trajectory suggests that the probiotic’s effect on vitamin K status may occur relatively early and then plateau, while fluctuations in the placebo group over time may obscure longer term differences. These temporal dynamics highlight the need for longer and larger trials to determine the stability and durability of probiotic effects on vitamin K metabolism.
To the best of our knowledge, this is the first study to investigate the effect of MK producing probiotics on vitamin K status. We can therefore not compare to other studies. Nevertheless, many studies investigated the effect of MK-7 supplementation on vitamin K status. These studies showed a 17-40% improvement of vitamin K status as measured by dp-ucMGP with a dosage of 180 μg/day MK-7 (Caluwe et al., 2014; Dalmeijer et al., 2012; Theuwissen et al., 2012; Westenfeld et al., 2012). Our results in the intervention group are in line with these studies, but our findings show a slightly weaker effect on dp-ucMGP. These differences can be explained by a relatively healthy study populations compared with populations of CKD patients, but the mode of supplementation might also play a role. All earlier studies supplemented MK-7 with a natto-derived supplement dissolved in oil, which is shown to have a high bioavailability (Schurgers et al., 2007). We used a probiotics supplement with MK producing bacterial strains. It is likely that bioavailability is lower for this supplement due to loss of probiotics during gastric passage (Valdes et al., 2018). In addition, the absorption and bioavailability of MKs in the gut is debated. Early reports suggested that up to 50% of the dietary requirement for vitamin K was fulfilled by intestinal production of MKs, based on measurements of vitamin K content in human livers (Suttie, 1995). However, the route of absorption of bacterially-produced MKs is still unclear. All vitamin K forms are absorbed in the small intestine via a process requiring bile salts (Suttie, 1995). Since bile salts are virtually absent in the colon where the majority of MKs are produced, this would suggest low absorption of these vitamin K forms in the colon (Conly and Stein, 1992). Indeed, a study by Ichihashi et al. showed that absorption of intestinally-produced MKs in rats is low and that absorption rates decrease markedly with the length of the side chain (Ichihashi et al., 1992). Our results suggest that MKs from probiotic strains are indeed partially absorbed, but the exact site of absorption is unknown. Of note, we also observed an increased MK-7 concentration in serum, which confirms absorption of MKs from probiotic sources.
Importantly, the investigational product did not contain free or purified MKs; all MKs were intracellular components of the probiotic strains themselves. This means that the observed effects may originate either from MKs naturally present within the bacterial biomass at ingestion or from MKs produced in vivo if the strains survive gastrointestinal passage. Because we did not assess colonisation, persistence, or metabolic activity of the strains, we cannot distinguish between these mechanisms. This uncertainty reflects the broader debate on whether bacterially produced MKs in the colon contribute meaningfully to systemic vitamin K status.
Our findings align with a growing body of literature suggesting that specific gut bacteria can synthesise long-chain menaquinones and may contribute to host vitamin K pool. Several species included in our formulation, such as Lactococcus lactis, Bacillus subtilis and Propionibacetirum freudenreichii, have been shown to produce MK-7 to MK-10 in vitro and in fermented foods (Bøe and Holo, 2020; LeBlanc et al., 2013; Morishita et al., 1999). Human data remain limited, but small studies have reported increases in circulating MKs following consumption of MK-producing strains or fermented foods rich in these bacteria (Karl et al., 2015; Walther et al., 2013). Our results extend this evidence by demonstrating that a multi-strain probiotic formulation can increase serum MK-7 and faecal MK-6/MK-7 concentrations in vivo. However, the magnitude of effect on dp-ucMGP was smaller than typically observed with direct MK-7 supplementation, suggesting that probiotic-derived MKs may be less efficiently absorbed or produced in lower quantities. Together, these findings highlight both the potential and the current limitations of leveraging MK-producing probiotics to modulate vitamin K status.
Other differences compared to earlier studies such as study populations may also play a role. Previous studies were conducted in healthy volunteers free from any chronic disease (Dalmeijer et al., 2012; Theuwissen et al., 2012) or patients with renal disease with a low vitamin K status as determined by high baseline dp-ucMGP concentrations of over 2800 pmol/l (Caluwe et al., 2014; Westenfeld et al., 2012). We conducted this study in people with an elevated cardiovascular risk who are expected to have a lower vitamin K status than the general population, since previous studies showed higher dp-ucMGP concentrations in those with CVD compared with healthy controls (Cranenburg et al., 2010). Our study population indeed had relatively high levels of dp-ucMGP in comparison to the proposed cutoff value of 400-500 pmol/l (Cranenburg et al., 2010; Riphagen et al., 2017), indicating a low vitamin K status. Since a low vitamin K status would likely produce larger effect sizes, it is unlikely that this explains the differences with other studies.
In addition to effects on dp-ucMGP, we also observed that MK-7 in serum and faeces and MK6 in faeces increased significantly after supplementation with MK producing probiotics compared with placebo. Since we observed no effect on phylloquinone levels in serum or faeces this supports the observed effect of probiotics on vitamin K status, as phylloquinone is not produced by probiotics. Although we did not detect any differences on other MK forms, MK-7 and MK-6 were among the most abundant MK species produced by the probiotic strains with the exception of MK-9. However, a previous study showed slow absorption of MK-9 in comparison with other MKs, which may in part explain the differential effects on MKs in serum and faeces (Schurgers and Vermeer, 2002).
Whether delivering MKs via probiotics offers advantages over direct MK supplementation remains uncertain. Probiotics may theoretically provide a sustained MK source if strains colonise and produce MKs in vivo, but given the unclear absorption of colonic MKs and the modest effect size compared with direct MK-7 supplementation, targeted MK supplementation remains the more predictable strategy. Probiotic-based MK delivery may nonetheless be relevant in populations already using probiotics for other indications.
The findings of this study show that MK producing probiotics can increase vitamin K status in people at elevated cardiovascular risk. Whether these results are generalisable to populations without cardiovascular risk or better vitamin K status needs to be determined in future studies. Also, MK supplements previously used in studies are likely more effective to improve vitamin K status in case targeted supplementation is needed to correct vitamin K deficiency. However, in populations using probiotic supplements for other indications such as bowel disease or antibiotic use, probiotic strains that produce MKs may also improve vitamin K status. This finding might be relevant specifically for an elderly population in nursing homes, but this requires further investigation in this population. This also suggests a contribution of the gut microbiome to vitamin K status, but currently little studies are available on the absorption, bioavailability and metabolism of bacterially produced MKs. In particular gastric bypass and site of absorption of MKs require further investigation. Although this study provides novel evidence that MK-producing probiotics can influence vitamin K status, the limited sample size means that the findings should be interpreted as exploratory. Larger studies are needed to confirm these results, explore dose-response relationships and determine whether specific strains or MK isoforms drive the observed effects. Although participants were selected based on elevated cardiovascular risk, this trial was not designed or powered to detect changes in cardiovascular outcomes or risk markers. Dp-ucMGP was chosen as a mechanistic biomarker of extra-hepatic vitamin K status rather than a clinical endpoint. Nevertheless, improving vitamin K status in individuals at elevated cardiovascular risk is clinically relevant, given the strong associations between dp-ucMGP, vascular calcification and cardiovascular diseases (Cranenburg et al., 2010; Mayer et al., 2014). Future studies with larger sample sizes, longer follow-up and dedicated cardiovascular endpoints are needed to determine whether probiotic-induced improvements in vitamin K status translate into cardiovascular benefit.
In conclusion, supplementation with MK producing probiotics increases vitamin K status as measured by dp-ucMGP in people at elevated cardiovascular risk. These findings were also reflected by increased serum and faecal MK concentrations. Whether supplementation with probiotics may also improve functional outcomes needs to be further investigated in longer term studies in larger sample sizes.
Corresponding author; e-mail: m.muilwijk@amsterdamumc.nl
These authors contributed equally to the manuscript
Acknowledgements
The authors would like to acknowledge the study participants for their contribution. This work was funded by Health∼Holland, grant number 2006241. Winclove Probiotics b.v. contributed both in cash and in kind; they provided the probiotics and placebo sachets and randomised the trial participants. Winclove Probiotics b.v. did not receive any participant information, nor did they have a role in the collection, analysis or interpretation and writing of the report, or the decision to submit the article for publication.
Authors’ contribution
Conceptualisation: Joline Beulens, Stephan Bakker; Methodology: Joline Beulens, Stephan Bakker, Mirthe Muilwijk, Sanne Kremers, Leon Schurgers; Formal analysis and investigation: Mirthe Muilwijk, Sanne Kremers; Writing – original draft preparation: Joline Beulens, Mirthe Muilwijk; Writing – review and editing: Joline Beulens, Mirthe Muilwijk, Sanne Kremers, Stephan Bakker, Leon Schurgers; Funding acquisition: Joline Beulens, Stephan Bakker; Supervision: Joline Beulens, Mirthe Muilwijk.
Conflict of interest
L.J. Schurgers received research funding from Boehringer Ingelheim, Gnosis by Lesaffre, Bayer, and IDS not related to this work, and is a stockholder in Coagulation Profile. The other authors have no relevant financial or non-financial interests to disclose.
Data availability
Our data contains identifying and sensitive participant information, and therefore cannot be shared publically as imposed by the ethics committee. The medical ethics committee of our institution considers that these data cannot be anonymised but only pseudonymised; this data is still considered personal data. The data is however available upon reasonable request by contacting the board of the Hoorn Studies; hoornstudy@vumc.nl or www.hoornstudies.com.
Full trial protocol
The full trial protocol has been assessed by the Medical Ethical Committee from VUmc, registration number NL71758.029.19 before commencement of the study, and is available upon reasonable request by contacting the board of the Hoorn Studies; hoornstudy@vumc.nl or www.hoornstudies.com.
References
Beulens, J.W., Booth, S.L., van den Heuvel, E.G., Stoecklin, E., Baka, A. and Vermeer, C., 2013. The role of menaquinones (vitamin K(2)) in human health. British Journal of Nutrition 110: 1357-1368. https://doi.org/10.1017/S0007114513001013
Booth, S.L., Broe, K.E., Gagnon, D.R., Tucker, K.L., Hannan, M.T., McLean, R.R., Dawson-Hughes, B., Wilson, P.W., Cupples, L.A. and Kiel, D.P., 2003. Vitamin K intake and bone mineral density in women and men. American Journal of Clinical Nutrition 77: 512-516. https://doi.org/10.1093/ajcn/77.2.512
Cranenburg, E.C., Koos, R., Schurgers, L.J., Magdeleyns, E.J., Schoonbrood, T.H., Landewe, R.B., Brandenburg, V.M., Bekers, O. and Vermeer, C., 2010. Characterisation and potential diagnostic value of circulating matrix Gla protein (MGP) species. Thrombosis and Haemostasis 104: 811-822. https://doi.org/10.1160/TH09-11-0786
Dalmeijer, G.W., van der Schouw, Y.T., Magdeleyns, E., Ahmed, N., Vermeer, C. and Beulens, J.W., 2012. The effect of menaquinone-7 supplementation on circulating species of matrix Gla protein. Atherosclerosis 225: 397-402. https://doi.org/10.1016/j.atherosclerosis.2012.09.019
EFSA Panel on Biological Hazards, Koutsoumanis, K., Allende, A., Alvarez-Ordonez, A., Bolton, D., Bover-Cid, S., Chemaly, M., De Cesare, A., Hilbert, F., Lindqvist, R., Nauta, M., Nonno, R., Peixe, L., Ru, G., Simmons, M., Skandamis, P., Suffredini, E., Cocconcelli, P.S., Fernandez Escamez, P.S., Prieto Maradona, M., Querol, A., Sijtsma, L., Suarez, J.E., Sundh, I., Barizzone, F., Correia, S. and Herman, L., 2024. Update of the list of qualified presumption of safety (QPS) recommended microbiological agents intentionally added to food or feed as notified to EFSA 19: Suitability of taxonomic units notified to EFSA until September 2023. EFSA Journal 22: e8517. https://doi.org/10.2903/j.efsa.2024.8517
Furuichi, K., Hojo, K., Katakura, Y., Ninomiya, K. and Shioya, S., 2006. Aerobic culture of Propionibacterium freudenreichii ET-3 can increase production ratio of 1,4-dihydroxy-2-naphthoic acid to menaquinone. Journal of Biosciences and Bioengineering 101: 464-470. https://doi.org/10.1263/jbb.101.464
Huang, W., Li, J., Zhu, Q., Lv, J., Zhu, R., Pu, C., Zhao, H., Fu, G. and Zhang, D., 2024. Increasing vitamin K(2) synthesis in Bacillus subtilis by controlling the expression of MenD and stabilizing MenA. Journal of Agricultural and Food Chemistry 72: 22672-22681. https://doi.org/10.1021/acs.jafc.4c07385
Karl, J.P., Fu, X., Wang, X., Zhao, Y., Shen, J., Zhang, C., Wolfe, B.E., Saltzman, E., Zhao, L. and Booth, S.L., 2015. Fecal menaquinone profiles of overweight adults are associated with gut microbiota composition during a gut microbiota-targeted dietary intervention. American Journal of Clinical Nutrition 102: 84-93. https://doi.org/10.3945/ajcn.115.109496
Mayer, O., Jr., Seidlerová, J., Bruthans, J., Filipovský, J., Timoracká, K., Vaněk, J., Cerná, L., Wohlfahrt, P., Cı́fková, R., Theuwissen, E. and Vermeer, C., 2014. Desphospho-uncarboxylated matrix Gla-protein is associated with mortality risk in patients with chronic stable vascular disease. Atherosclerosis 235: 162-168. https://doi.org/10.1016/j.atherosclerosis.2014.04.027
Östlund-Lagerström, L., Kihlgren, A., Repsilber, D., Björkstén, B., Brummer, R.J. and Schoultz, I., 2016. Probiotic administration among free-living older adults: a double blinded, randomized, placebo-controlled clinical trial. Nutrition Journal 15: 80. https://doi.org/10.1186/s12937-016-0198-1
PASS, 2017. PASS 15 Power Analysis and Sample Size Software. NCSS, LLC. Kaysville, Utah, USA.
Riphagen, I.J., Keyzer, C.A., Drummen, N.E.A., de Borst, M.H., Beulens, J.W.J., Gansevoort, R.T., Geleijnse, J.M., Muskiet, F.A.J., Navis, G., Visser, S.T., Vermeer, C., Kema, I.P. and Bakker, S.J.L., 2017. Prevalence and effects of functional vitamin K insufficiency: The PREVEND Study. Nutrients 9: 1334. https://doi.org/10.3390/nu9121334
Salminen, S., Collado, M.C., Endo, A., Hill, C., Lebeer, S., Quigley, E.M.M., Sanders, M.E., Shamir, R., Swann, J.R., Szajewska, H. and Vinderola, G., 2021. The International Scientific Association of Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of postbiotics. Nature Reviews Gastroenterology and Hepatology 18: 649-667. https://doi.org/10.1038/s41575-021-00440-6
Suttie, J.W., 1995. The importance of menaquinones in human nutrition. Annual Review of Nutrition 15: 399-417. https://doi.org/10.1146/annurev.nu.15.070195.002151
Theuwissen, E., Cranenburg, E.C., Knapen, M.H., Magdeleyns, E.J., Teunissen, K.J., Schurgers, L.J., Smit, E. and Vermeer, C., 2012. Low-dose menaquinone-7 supplementation improved extra-hepatic vitamin K status, but had no effect on thrombin generation in healthy subjects. British Journal of Nutrition 108: 1652-1657. https://doi.org/10.1017/S0007114511007185
Westenfeld, R., Krueger, T., Schlieper, G., Cranenburg, E.C., Magdeleyns, E.J., Heidenreich, S., Holzmann, S., Vermeer, C., Jahnen-Dechent, W., Ketteler, M., Floege, J. and Schurgers, L.J., 2012. Effect of vitamin K2 supplementation on functional vitamin K deficiency in hemodialysis patients: a randomized trial. American Journal of Kidney Diseases 59: 186-195. https://doi.org/10.1053/j.ajkd.2011.10.041






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}