Abstract
Epidemiologic studies have implicated the gut microbiota in acute kidney injury (AKI), but the causal relationship is unclear. Using Mendelian randomisation, we explored the causal role of gut microbiota in the development of acute kidney injury after excluding confounding and reverse causality. Mendel randomised (MR) study was conducted using data from intestinal microbiota and genome-wide association studies (GWAS) disease of acute kidney injury and the sequencing data of case-control study confirmed this finding. The summary statistics of intestinal microbiota (n = 13,266) conducted by MiBioGen Alliance was taken as the exposure, while the statistics of acute kidney injury obtained from FinnGen Alliance data (2,383 cases and 212,841 controls) were taken as the results. A total of 42 patients were included in this case-control study. Evidence for the protective causal associations of the genus Flavonifractor id.2059 with AKI was found in inverse variance weighting (odds ratio = 0.48 [95% confidence interval, 0.32-0.72];
1 Introduction
Acute kidney injury (AKI) is a common clinical acute complication that causes approximately 2 million deaths worldwide every year and is a major public health problem affecting millions of patients worldwide (Ronco et al., 2019). Septic AKI (S-AKI) is the most common AKI syndrome in the intensive care unit (ICU), accounting for approximately half of all AKI cases (Bellomo et al., 2017; Wang et al., 2012). In addition, the rate of missed diagnosis of AKI in hospitalised adult patients is 52.7% (Cheng et al., 2017), the mortality rate of AKI in critically ill patients is as high as 49.8% (Er et al., 2020) and the long-term prognosis of S-AKI is poor. Research indicates that AKI impacts remote organs through mechanisms such as inflammatory responses, metabolic and hemodynamic changes and the neuroendocrine system. When the kidneys are damaged, remote organs may also be affected (Monard et al., 2023). Given the complexity of AKI diagnosis and treatment, it is crucial to pursue new potential therapeutic approaches.
Recently, changes in gut bacteria termed ‘gut dysbiosis’ have been associated with dysfunction of distant organs, including the heart, lung, kidney and brain (Saranya et al., 2023). Intestinal dysbiosis can also aggravate kidney injury (Chou et al., 2022). Therefore, the identification of intestinal factors that are closely related to changes in the gastrointestinal microbiota, leading to the abnormal intestinal pathogenesis of AKI, especially the intestinal microbiota, may be of great significance for the early identification and optimisation of the clinical diagnosis and treatment of AKI. Several studies have investigated the relationship between the gut microbiota and AKI (Gharaie et al., 2023; Kim et al., 2021; Lee et al., 2021; Zhu et al., 2021). However, most of these studies are case-control studies based on sample size and there are residual confounding factors, such as genetic background, age, sex, weight and race. These intrinsic factors affecting the gut microbiota may interfere with causal inference.
In this study, we used a two-sample Mendelian randomisation method to investigate the role of the gut microbiota in the development of AKI. We further validated this relationship by a clinical case-control study based on 16S rRNA sequencing data, hoping to provide a theoretical basis for the early prevention, diagnosis and treatment of AKI.
2 Materials and methods
Mendelian randomisation
Mendelian randomisation (MR) is a data analysis technique in epidemiological research that uses single nucleotide polymorphisms (SNPs) as instrumental variables (IVs) to evaluate the causal relationship between exposure factors and outcomes (Davey Smith et al., 2014).
The study strictly followed the three core assumptions of Mendelian randomisation (Emdin et al., 2017): (1) the selected instrumental variables were strongly associated with exposure, (2) the instrumental variables were not associated with any confounding factors and (3) the instrumental variables could affect the outcome only through exposure (Figure 1).

Schematic diagram of Mendelian randomisation (MR). Three assumptions should be met, as follows: Assumption 1 – The SNPs should be closely related to exposures; Assumption 2 – The IVs selected are supposed to be independent of confounders; Assumption 3 – SNPs should influence the outcomes just through the exposure. IVs = instrumental variables; SNPs = single-nucleotide polymorphisms.
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
Ethics approval and consent to participate
Mendelian randomisation studies used publicly available genome-wide association study data; ethical clearance and informed consent were provided at the time of the initial study. The trial was conducted in the Department of Critical Care Medicine, the First Affiliated Hospital of Harbin Medical University, Heilongjiang Province, China and was approved by the Ethics Committee of the First Affiliated Hospital of Harbin Medical University (IRB-AF/SC-04/02.0). Written informed consent was obtained from an authorised representative of the patients.
Sources of genome-wide association study summary data
Gut microbiota
The data of the gut microbiota study came from the latest genome-wide association study (GWAS) of the Mibiogen consortium (Kurilshikov et al., 2021; MiBioGen consortium, 2022), which included 18,340 individuals from 24 cohorts, most of whom had European ancestry (n = 13,266), targeting variable regions V4, V3-V4 and V1-V2 of the 16S rRNA gene to profile the microbial composition and to conduct taxonomic classification using direct taxonomic binning. In this study, the genus was the lowest taxonomic level and 131 genera with an average abundance greater than 1% were identified. After removing 12 unknown genera, this study finally included 119 genus-level taxa for analysis (Kurilshikov et al., 2021).
Acute kidney injury
GWAS summary statistics for AKI were obtained from the FinnGen Consortium R7 publication data (FinnGen, 2022; Kurki et al., 2022). After adjusting for potential covariates such as sex, age and other covariates, a total sample was obtained, including data from 2,383 cases and 212,841 controls, all of which were Finnish adult subjects (Kurki et al., 2022).
Selection of instrumental variables
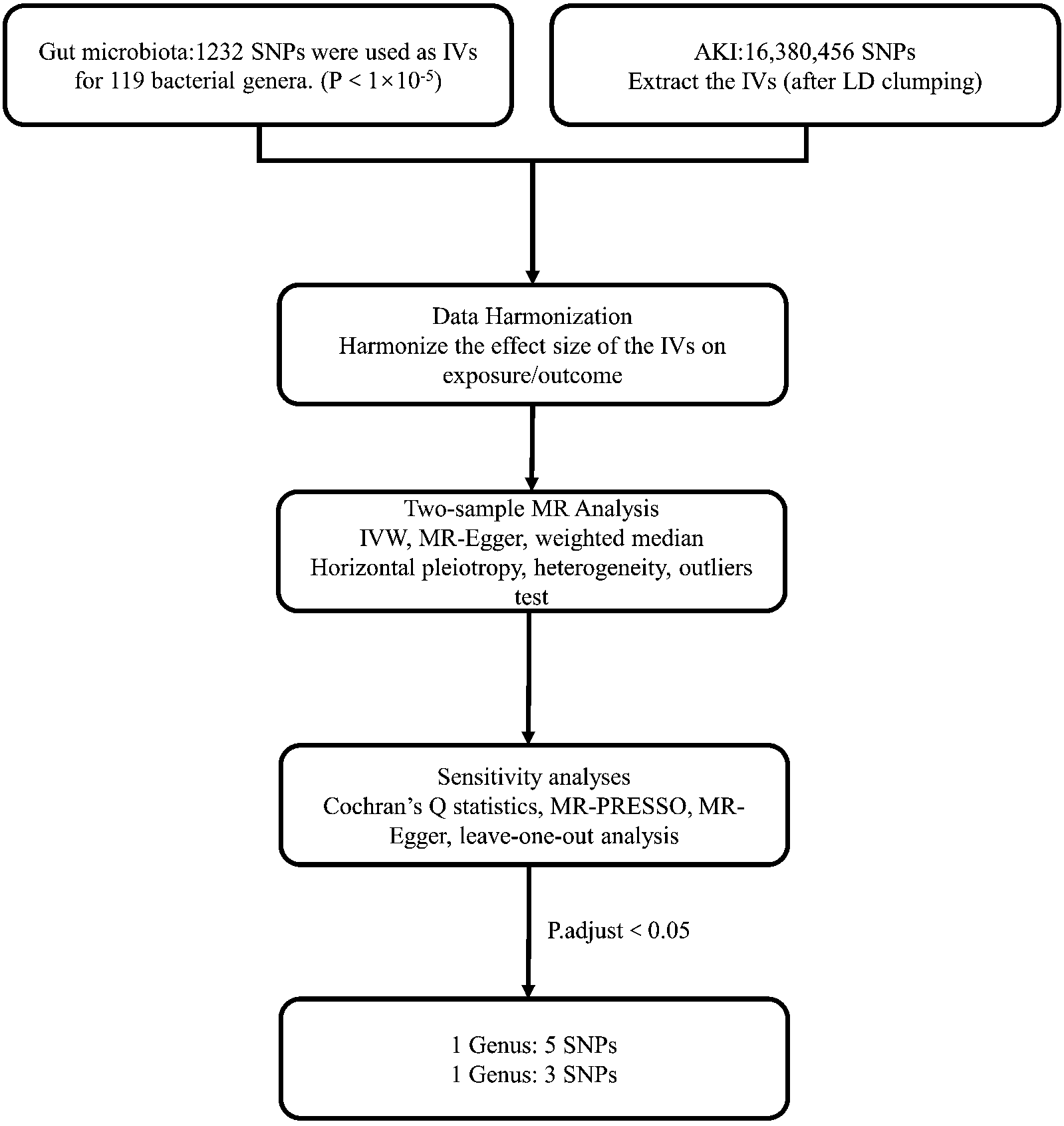
To ensure data robustness and accuracy, we implemented a rigorous screening process on publicly available genome-wide association study data from the Mibiogen consortium. We followed the steps shown in Figure 2. First, SNPs associated with each gut microbiota category were selected as instrumental variables. Two thresholds were used to select instrumental variables. At the beginning, we used a genome-wide statistical significance threshold (5 × 10−8) to screen instrumental variables, but only a few SNPs met the significance threshold, so we selected 1 × 10−5 with broad significance levels to screen instrumental variables to include more genetic tools to explore potential associations and perform sensitivity analyses. This is consistent with previous studies (Kurilshikov et al., 2021; Yu et al., 2023). Second, SNPs that matched GWAS AKI exposure were extracted. Third, SNPs with a minimum allele frequency (MAF) ≤ 0.01 were excluded. Fourth, we coordinated alleles for SNPs affecting gut microbiota and acute kidney injury size. Incompatible alleles and palindromic sequences were removed. Fifth, in the case of SNPs for which no results were available in GWAS data, we searched for qualified proxy SNPs in R through the LDlink online platform (1000 Genomes Project Consortium et al., 2015). Sixth, linkage disequilibrium (LD) analysis was conducted based on the European 1000 Genomes Project (LDlink online platform, 2023) and the cluster distance was set to 10,000 kb. Nonconforming single nucleotide polymorphisms (SNPs) (R2 < 0.001). We then formed a new merged result without the palindromic sequence. F-statistics were used to assess the strength of the relationship between instrumental variables and exposure. If F < 10, then a weak instrumental variable is assumed. The F-value was calculated as follows: [R2 ∗ (n − k − 1)]∕[k ∗ (1 − R2)], where R2 represents the proportion of variance explained by genetic instruments, n represents the sample size and k represents the number of instruments (Staiger, 1997). Seventh, SNPs significantly associated with confounding factors were examined and excluded through the PhenoScanner GWAS database (PhenoScanner GWAS database, 2023).
Mendelian analysis flow chart. AKI = acute kidney injury; SNPs = single-nucleotide polymorphisms; MR = Mendelian randomisation; IVs = instrumental variables; IVW = inverse-variance weighted; LD = linkage disequilibrium.
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
Mendelian analysis
After the above instrumental variables were selected, we used inverse variance weighted (IVW), weighted median and MR Egger as the main analysis methods of MR and the results of the three methods were measured by OR value. A P-value < 0.05 was considered to be significantly significant. The IVW method is an effective analysis under the basic premise that all genetic variants are valid instrumental variables, which has a strong ability to detect causality (Burgess et al., 2016). If up to 50% of the instrumental variables are invalid, the weighted median can also correctly estimate the causal relationship (Hartwig et al., 2017). MR-Egger regression allows all genetic variants to have pleiotropic effects but requires pleiotropic effects to be independent of the variant exposure association (Bowden et al., 2015).
To assess the robustness of the MR results, we performed a series of sensitivity analyses. First, we used MR–Egger and inverse variance weighting to evaluate the heterogeneity of the results and calculated Cochran’s Q to evaluate the magnitude of heterogeneity (Greco et al., 2015). Second, for pleiotropy, we used two methods: one was to test horizontal pleiotropy by the MR Egger intercept method and the other was to evaluate the horizontal pleiotropy of instrumental variables by the MR-PRESSO global test (Verbanck et al., 2018).
Finally, we visually analysed the specific MR results by scatter plots, funnel plots and forest plots. All data analyses were performed in RStudio version 4.2.2. The R packages used were TwoSampleMR version 0.5.6, MRInstruments version 0.3.2, MRPRESSO version 1.0 and data. table version 1.14.8.
Clinical case-control study
Participant recruitment
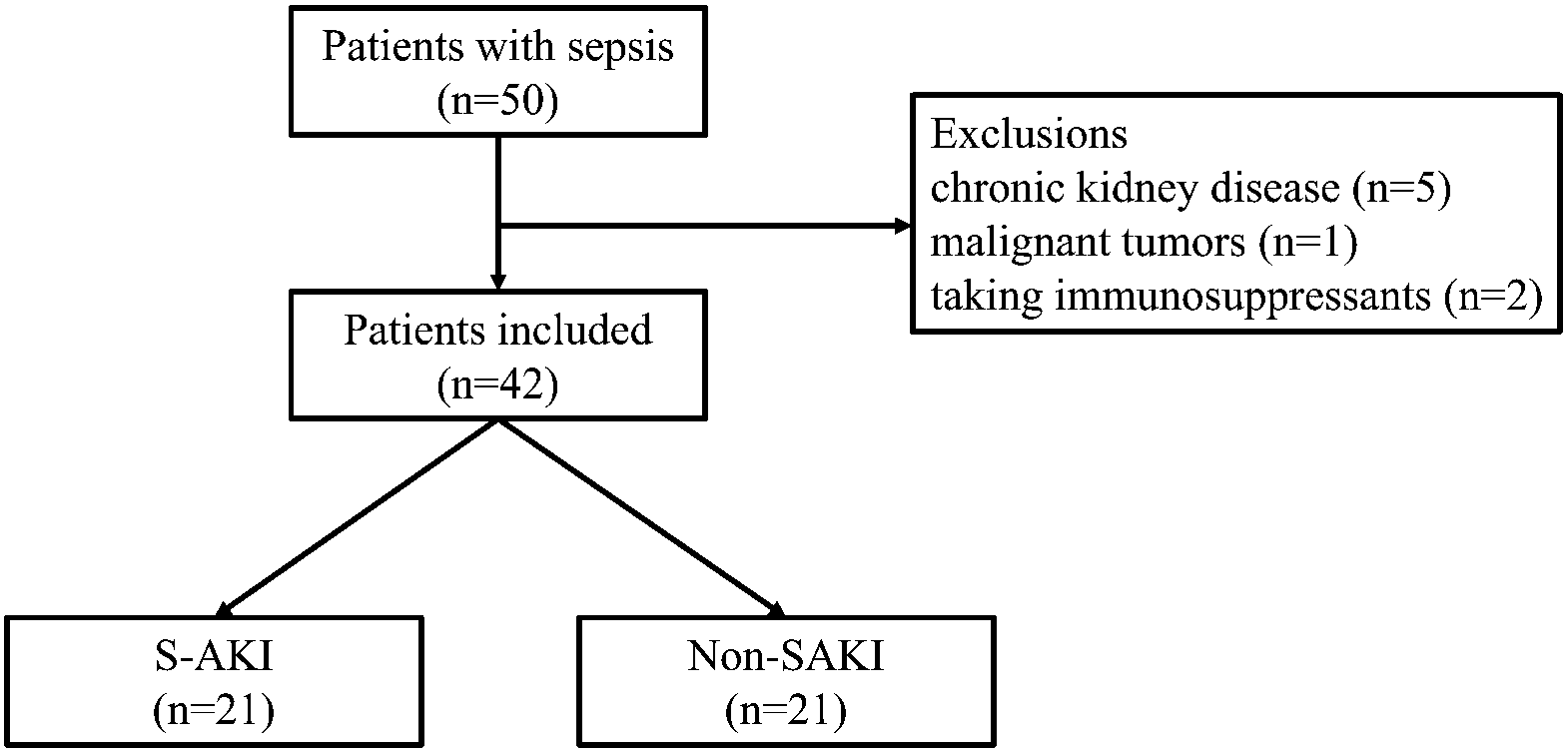
We identified 50 patients with newly diagnosed sepsis from the intensive care unit of the First Affiliated Hospital of Harbin Medical University (Heilongjiang, China) from December 2021 to September 2022. Patients were selected based on the third international consensus definition of sepsis (Singer et al., 2016). After exclusion of chronic kidney disease, previous cancer diagnoses and taking immunosuppressants, 42 patients were included in our study (Figure 3). AKI was diagnosed according to the KDIGO clinical practice guidelines (Acute Kidney Injury Work Group KDIGO Clinical Practice Guideline for Acute Kidney Injury, 2012). Specifically, AKI was diagnosed based on an increase in serum creatinine (SCr) of 0.3 mg/dl (≥26.5 μmol/l) within 48 h after septic patients are hospitalised. All the 21 patients with S-AKI included in the study were anuric AKI.
Flowchart of the enrolled patients.
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
The clinical data of patients on the day of diagnosis were collected, including age, sex, creatinine, length of ICU stay, SOFA score, APACHE II score, C-reactive protein, procalcitonin (PCT), PH, lymphocyte percentage and other clinical information. The 28-day survival of patients with sepsis was followed up.
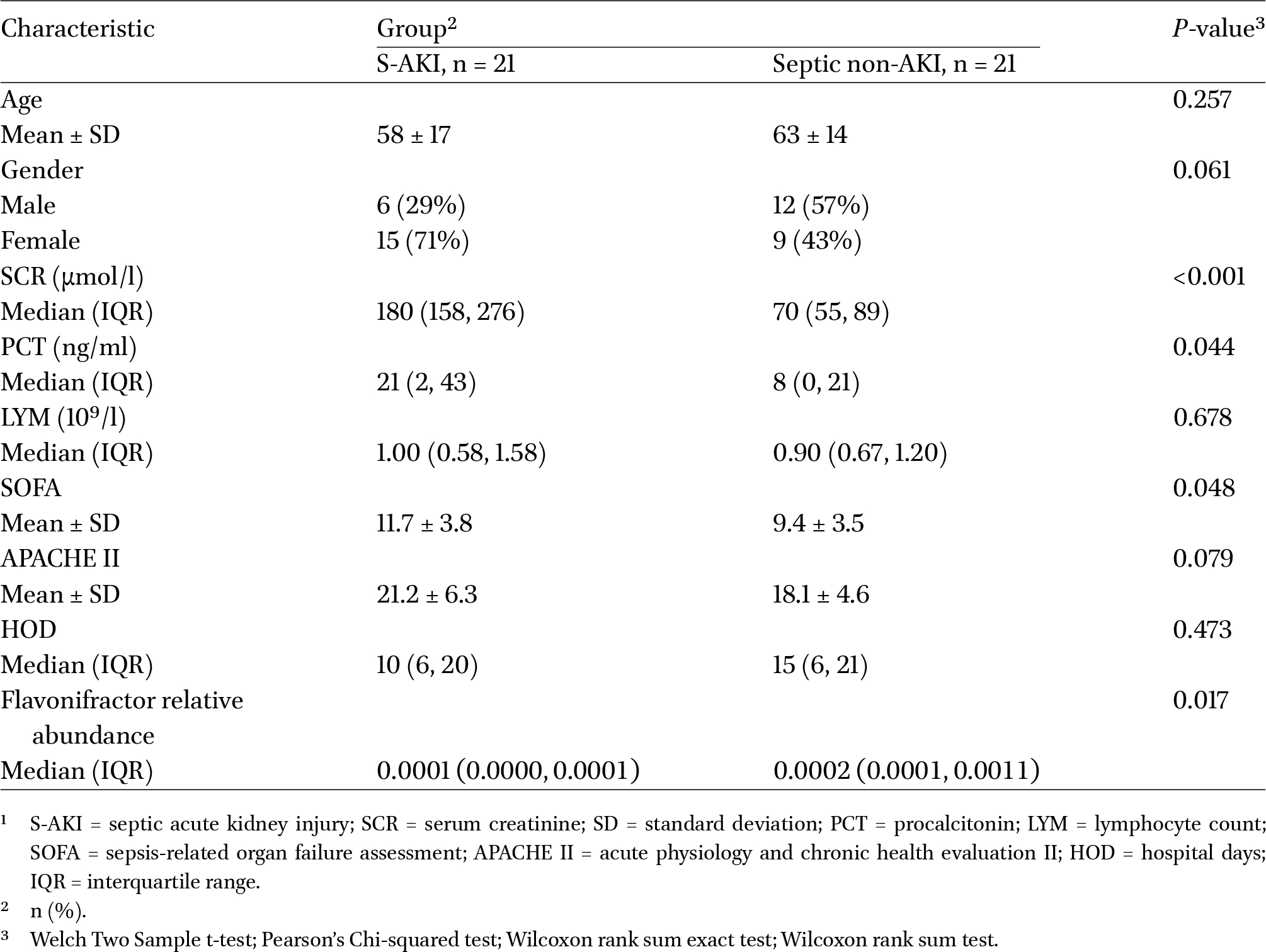
The study protocol was approved by the ethics committee of the First Affiliated Hospital of Harbin Medical University (IRB-AF/SC-04/02.0). All participants signed informed consent. Clinical characteristics of the patients at baseline are shown in Table 1.
Demographic and clinical characteristics of participants.1
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
Stool specimen collection
For patients who met the inclusion criteria, specimens were collected on the first day of diagnosis. In brief, the patient was kept in a detectable position on the left side and a cotton swab free of RNase and DNase was inserted 2 to 3 cm into the rectal sphincter, rotated 360°, placed for approximately 20 s, removed and checked for successful sampling. After successful collection, the swab was placed in a protective tube made of polystyrene. The collected samples were immediately snap-frozen in liquid nitrogen and stored in a −80 °C freezer.
16S rRNA and bioinformatics analysis of intestinal microorganisms
DNA was extracted by corresponding DNA extraction kits (QIAamp Fast DNA Stool Mini Kit, No. 51604; Qiagen, Hilden, Germany). DNA integrity and purity were assessed by 1% agarose gel electrophoresis. DNA concentration and purity were determined by NanoDrop One (Thermo Fisher Scientific, Waltham, MA, USA). The extracted DNA was used as a template for PCR amplification and the V3-V4 sequencing region was selected for amplification. Bar-coded primers (cord: 341F 5′-CCTACGGGRSGCAGCAG-3′ and 806R 5′-GGACTACVVGGGTATCTAATC-3′, Invitrogen, Carlsbad, CA, USA) and Premistaq (Takara Biotechnology, Dalian, China) were used for PCR amplification. PCR was performed as described in previous study (Li et al., 2024). One microliter of each primer (10 μm) and 3 μl of DNA (20 ng/μl) template in a 50 μl volume were amplified by the following thermal cycling conditions: 5 min at 94 °C for initialisation; ‘30 cycles of denaturation at 94 °C for 30 s, annealing at 52 °C for 30 s and extension at 72 °C for 30 s’; this was followed by a final extension at 72 °C for 10 min. The PCR instrument was a Bio-Rad S1000 (Bio-Rad Laboratory, Hercules, CA, USA). According to the Neb next Ultra TMDNA Library PrepKit for lllumina (New England Biolabs, Ipswich, MA, USA) standard methods for the following library construction, the MiSeq/HiSeq platform (Illumina, Inc., San Diego, CA, USA) was used to sequence the V3-V4 region. Sequencing data were analysed by base call analysis and converted to raw readings, resulting in sequencing reports.
Phylogenetic analysis of the 16S rRNA genes
Amplicon sequences from five representative species (OTU68, OTU2271, OTU2610, OTU2338 and OTU4147) were selected from the genus Flavonifractor. For each operational taxonomic unit (OTU), the nucleotide (nt) database of the National Center for Biotechnology Information (NCBI) was searched separately using BLASTN and screened to obtain 16S rRNA gene sequences (>1,300 nt in length) for the 20 most closely related type strains. These sequences were aligned using the SILVA Incremental Alignment Service (SINA) (https://www.arb-silva.de/aligner/) and corrected using trimAl (v1.4.rev15; parameter: -gappyout) to remove unreliable regions with large amounts of missing data (Capella-Gutiérrez et al., 2009; Pruesse et al., 2012) and the corrected alignment data were imported into IQ-TREE (v1.6.8) and phylogenetic trees constructed using the maximum likelihood method (Nguyen et al., 2015).
Sequencing data statistics
The Mann-Whitney test was used for the relative abundance of the gut microbiota between the septic AKI group and the septic non-AKI group and between the 28-day septic AKI survival group and the 28-day septic non-AKI death group. Clinical indicators and microbial relative abundance were investigated using correlation analysis and Spearman’s coefficient was used to illustrate the results. Analyses were performed in RStudio version 4.2.2. and IBM SPSS Statistics version 26 (Armonk, NY, USA).
3 Results
The association of increased relative abundance of gut microbiota with acute kidney injury.1
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
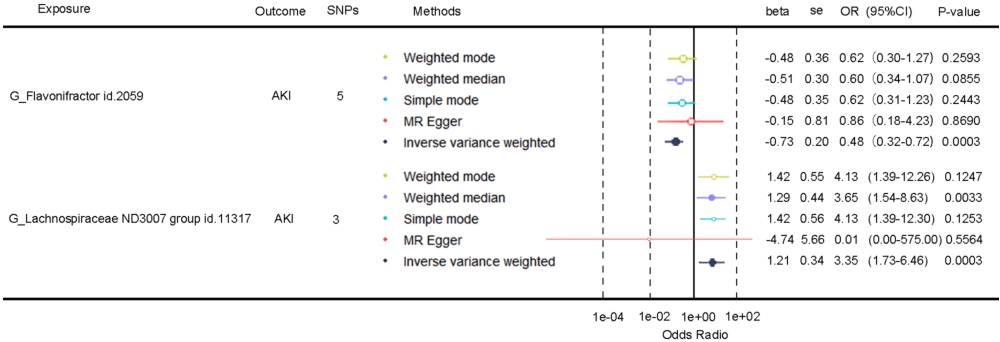
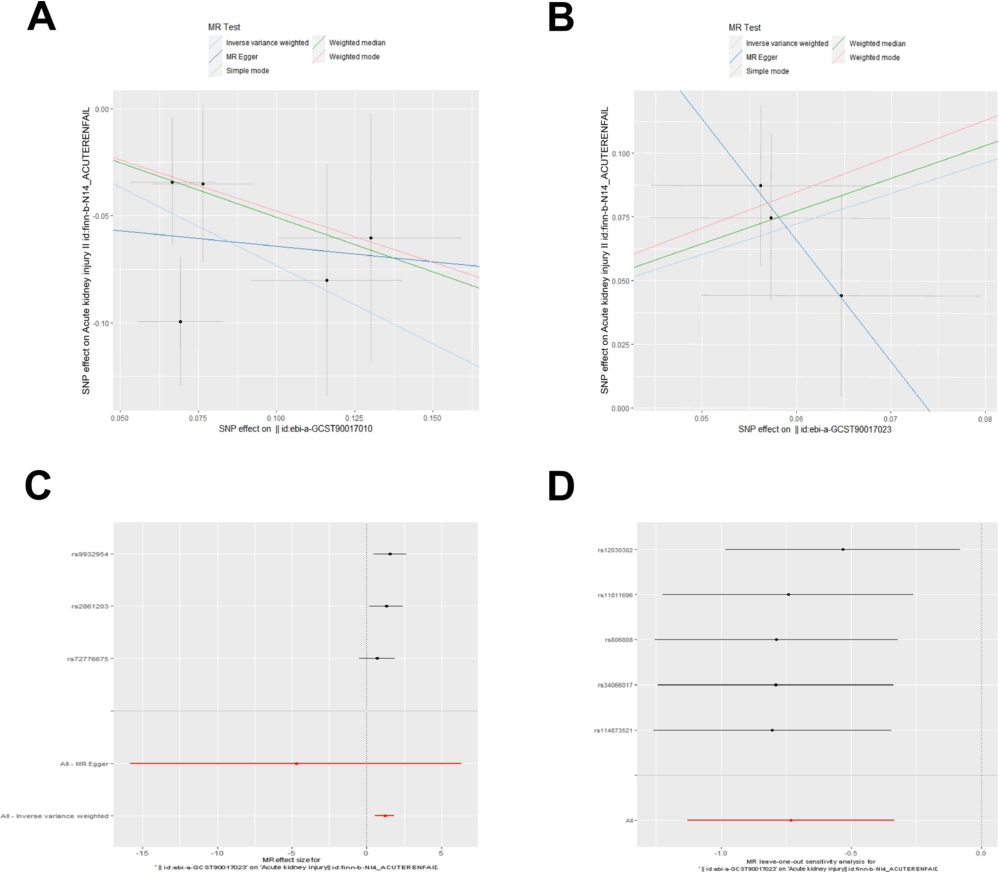
We mainly used the IVW method to determine whether there was a causal relationship between exposure and outcome, while MR-Egger and WM methods were used to avoid bias and scatter plots were presented (Figure 5A-B). We identified 2 taxa that are potentially causally related to AKI. genus Lachnospiraceae ND3007 group id.11317 showed a positive causal relationship [3.35 (1.73-6.46),
We further performed a sensitivity analysis. No heterogeneity was found by the Cochran Q test (Table 2). The MR–Egger intercept analysis and the MR-PRESSO global test did not identify potential horizontal pleiotropy (Table 2). The MR-PRESSO outlier correction test did not find outlier points. Finally, we performed a leave-one-out analysis (Figure 5C-D), which supported that the MR results were not influenced by a single SNP.
Clinical baseline demographic information and clinical characteristics
Stool samples were collected from a total of 42 participants in the case-control study. The sequencing variables did not meet the preconditions of ANOVA and t-tests, so the Mann-Whitney test was used. The baseline demographic and clinical characteristics of all participants are shown in Table 1.
Mendelian randomisation-clinical sequencing validation
Forest plot of the causal effects of the gut microbiota on acute kidney injury (AKI).
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
(A, B) Scatter and (C, D) leave-one-out sensitivity analysis of the association between the gut microbiota and acute kidney injury (AKI).
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
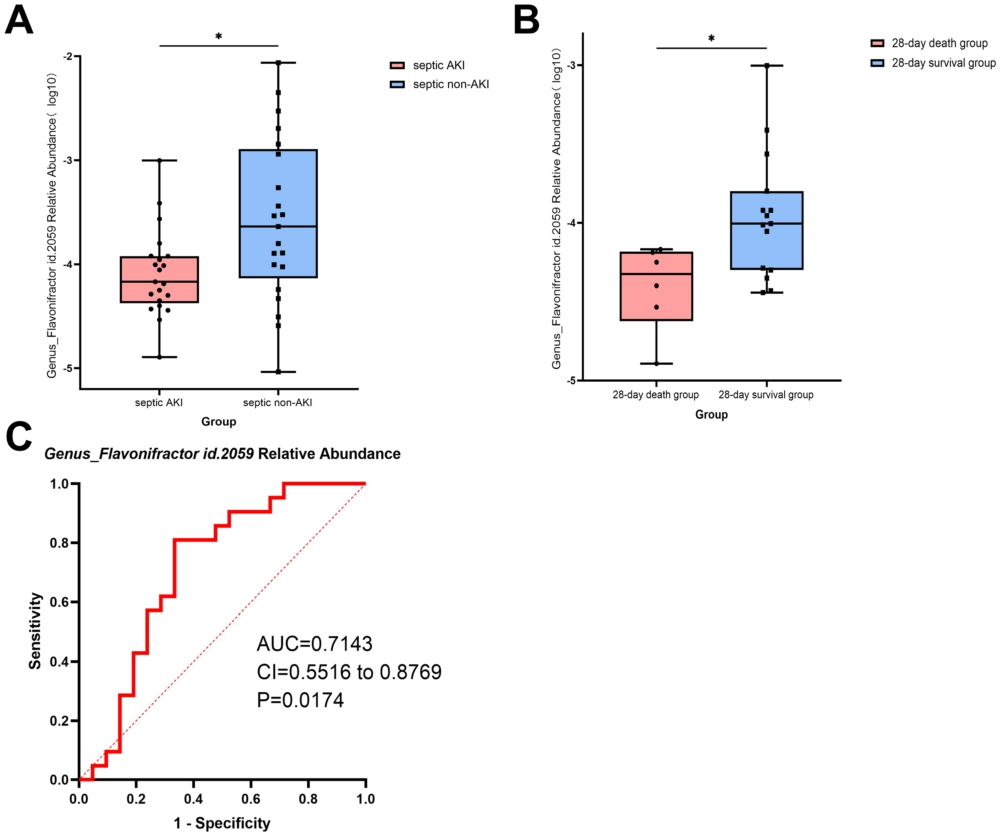
Data obtained from case-control studies were validated by Mendelian randomisation results. We extracted the relative abundance of genus Flavonifractor id.2059 expression for each participant and compared the difference in genus Flavonifractor id.2059 expression between the septic AKI group and the septic non-AKI group and between the 28-day septic AKI survival group and the 28-day septic non-AKI death group. The results showed that the relative abundance of the genus Flavonifractor id.2059 (
Bar plots to validate Mendelian randomisation. (A) Comparative relative abundance of the genus Flavonifractor in the septic acute kidney injury (AKI) group and septic non-AKI group; (B) Comparative relative abundance of the genus Flavonifractor in the 28-day survival group and 28-day death group. (C) The ROC curve of the prediction model of relative abundance of the genus Flavonifractor is described. *
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
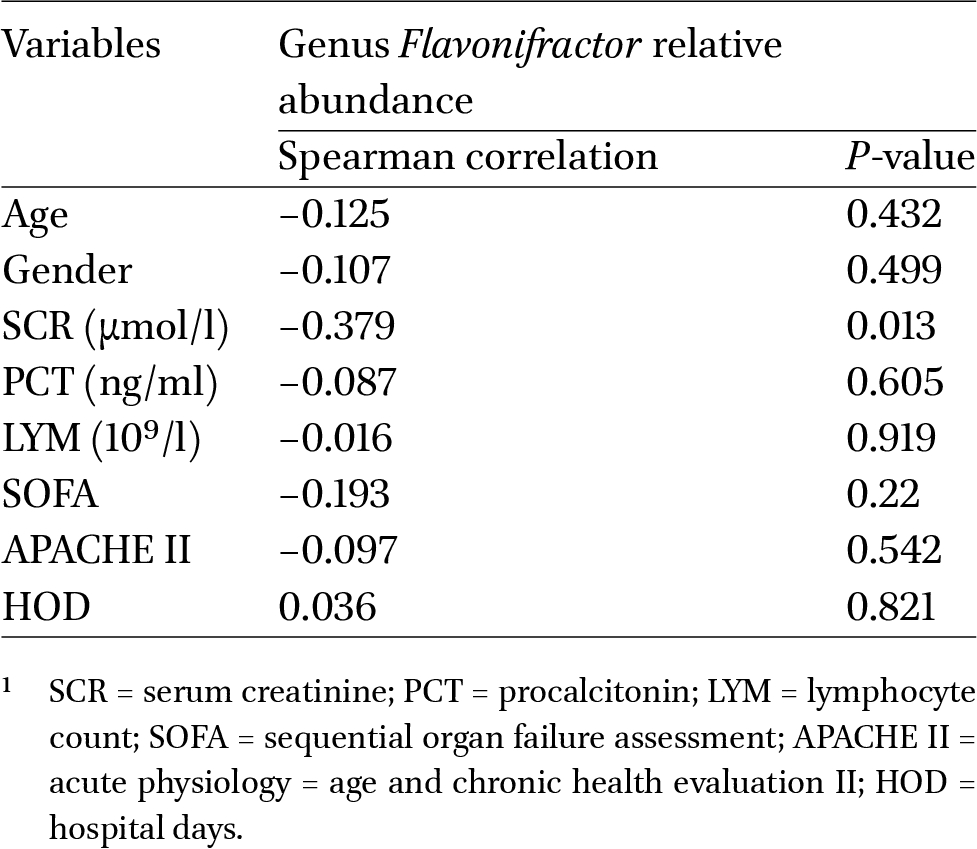
Correlation between relative abundance of genus Flavonifractor id.2059 and clinical variables1
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
Phylogenetic analysis
The phylogenetic tree was constructed utilising the OTUs representing five distinctive species of the genus Flavonifractor (Figure 7). Bacteria belonging to the same genus were denoted with a uniform colour. Specifically, OTU68 is classified as Flavonifractor and exhibits the most proximate genetic relationship with HQ455040.1334-739, sharing a genetic similarity of 100%. Conversely, OTU2271 belongs to the genus Pseudoflavonifractor and has the closest genetic kinship with LT598575.1365-770, also with a genetic similarity of 100%. The remaining OTUs, namely OUT2338, OTU2610 and OTU4147, remain unclassified. The above results indicate that the genetic relationship at the genus level of Flavonifractor needs to be further explored.
4 Discussion
In this study, we used Mendelian randomisation to determine the protective causal effect of the genus Flavonifractor id.2059 on AKI and the correlation between its relative abundance and creatinine value was also found to be significant. To the best of our knowledge, this is the first report to analyse the causal relationship between gut microbiota and AKI based on a GWAS dataset. These findings will be useful for the study of AKI prevention and clinical management.
Mendelian randomisation eliminates possible confounding in the population and is based on the random allocation principle of biological genetics, which makes the results more robust and reliable. After obtaining the MR results, we further validated these results with a case-control study. We successfully analysed the difference in the relative abundance of the genus Flavonifractor id.2059 between the septic AKI group and the septic non-AKI group. Unfortunately, due to the limitation of sequencing results, we could not verify the difference in the relative abundance of the genus Lachnospiraceae ND3007 group id.11317 among different groups.
More than 1000 species of bacteria colonise the human gut and shape the composition of the gut microbiota (Gilbert et al., 2018). Studies have found that the intestinal microbiota plays an important role in maintaining gastrointestinal homeostasis by participating in the establishment of the immune barrier and mediating the inflammatory response and nutrient metabolism. The gut microbiota affects various organs and systems in the human body, including the kidneys. Although the gut microbiota mainly targets chronic injury, AKI is also affected by the gut microbiota (Kobayashi et al., 2021). Gut barrier disruption, immune and soluble mediators of microbiome effects and dysbiosis are associated with the pathogenesis of acute kidney injury (Gong et al., 2019). Using Mendel randomisation, a study identified genera Escherichia-Shigella and Howardella as potential risk factors for chronic renal failure and proposed potential intervention measures for these two genera to slow down the progress of chronic renal failure (Liu et al., 2024). Transplantation of Enterobacteriaceae into these germfree mice reduced kidney insufficiency and histological damage and altered the composition of kidney lymphocytes, demonstrating the renoprotective role of the gut microbiota (Jang et al., 2009). In addition, the gut microbiota produces SCFAs from indigestible dietary fibre, such as acetate, propionate and butyrate, which are involved in the inflammatory response and have been found to reduce kidney injury (Andrade-Oliveira et al., 2015; Felizardo et al., 2019; Machado et al., 2012).
Phylogenetic tree based on genome sequences, showing the phylogenetic relationship between genus Flavonifractor and the closely related species.
Citation: Beneficial Microbes 15, 6 (2024) ; 10.1163/18762891-bja00032
Flavonifractor plautii (FP) is a gram-positive anaerobe of the genus Clostridium and is involved in catechin metabolism (Carlier et al., 2010). Oral FP can suppress Th2 immune responses by incorporation of MLNs and/or induction of changes in the gut microbiota; therefore, FP may help alleviate antigen-induced Th2 immune responses (Ogita et al., 2020). In a human faecal metagenomic sequencing study, FP was shown to be significantly elevated in abundance and centrality in normal controls, which were absent in the microbial communities of subjects with elevated arterial stiffness. This suggests that FP may play a role in preventing increased arterial stiffness (Luo et al., 2023). In addition, one study also found that oral Flavonifractor plautii can promote the recovery of acute colitis in mice by inhibiting IL-17 (Mikami et al., 2021). In addition, the study also confirmed that the application of green tea increased the abundance of FPs in the intestinal microbiota. However, the role of Flavonifractor in AKI has not been found. This suggests that more work is needed to determine the causal relationship and role of gut microbes, including Flavonifractor, in kidney injury diseases.
Treatments for AKI include management of the underlying disease, fluid balance, antibiotics and renal replacement (Yu et al., 2022). However, the relationship between gut microbiota and AKI remains unclear and few clinically relevant microbiota have been proposed. Our study validated the protective role of genus Flavonifractor in AKI using Mendelian randomisation and case-control studies, offering a new diagnostic and therapeutic approach.
Several studies have examined serum and urine to identify AKI markers, but have neglected the gut microbial perspective (Jia et al., 2022). We found that monitoring the abundance of genus Flavonifractor helps in the early detection of AKI (AUC = 0.7143, 95%CI: 0.5516-0.8769,
The advantage of this study lies in the first use of Mendelian analysis to explore the causal relationship between intestinal flora and AKI, which minimises potential confounding factors. Through clinical case-control studies, we have confirmed the causal relationship between genus Flavonifractor id.2059 and AKI. However, our study has some limitations. Firstly, the GWAS data on intestinal microbiota used in this Mendelian study originates from individuals of European ancestry, leaving unclear whether similar results can be obtained in other populations, thus posing limitations on the further validation of other causative bacteria. Moreover, while we have further validated the role of Flavonifractor id.2059 in S-AKI through clinical research, the small sample size and lack of consideration for AKI subtypes and long-term prognosis necessitate multi-centre, large-scale studies for further confirmation. Lastly, it is noteworthy that this Mendelian analysis only involves causal relationships at the genus level, disregarding potential causalities at other levels.
5 Conclusions
In summary, this study demonstrated a positive causal effect of the genus Flavonifractor on AKI and a case-control study showed that the relative abundance of the genus Flavonifractor id.2059 (
Corresponding authors; e-mail: drkaijiang@163.com; mingyan1970@126.com; changsongwangicu@163.com
These authors contributed equally.
Supplementary material
Supplementary material is available online at: https://doi.org/10.6084/m9.figshare.26661763
Table S1. Tool variable extraction table.
Table S2. Causal effect of exposure on outcome after correction of P-value.
Acknowledgements
The authors appreciate the MiBioGen consortium as well as the participants and investigators of the FinnGen study. The authors would also like to thank all the doctors, nurses and patients who participated in this case-control study.
Authors’ contribution
Yanqi Liu, Jiannan Zhang, Yuxin Zhou, Mingyan Zhao, Kaijiang Yu and Changsong Wang designed and performed the study. Nana Li, Yang Zhou, Feiyu Luan, Yue Li and Qianqian Zhang collected clinical samples and completed biological analysis. Mengyao Yuan, Yuhan Liu, Linqiong Liu, Yuchen Song, Lifeng Shen, Yu Xiao, Yuxi Liu, Yahui Peng and Xibo Wang undertook the statistical analyses. Yu Xin, Hongxu Li and Pengfei Huang interpreted the results. Yanqi Liu wrote the first draft of the manuscript. All the authors have read and approved the final manuscript.
Conflict of interest
The authors declare that they have no competing interests.
Data availability
The datasets analysed during the current study are available in the MiBioGen repository, https://mibiogen.gcc.rug.nl/ and the FinnGen repository, https://r7.finngen.fi/.
Funding
This study was supported by the National Natural Science Foundation of China-Regional Innovation and Development Joint Fund (U20A20366) and the Natural Science Foundation of Heilongjiang Province (JQ2021H003).
References
1000 Genomes Project Consortium, Auton, A., Brooks, L.D., Durbin, R.M., Garrison, E.P., Kang, H.M., Korbel, J.O., Marchini, J.L., McCarthy, S., McVean, G.A. and Abecasis, G.R., 2015. A global reference for human genetic variation. Nature 526: 68-74. https://doi.org/10.1038/nature15393
Andrade-Oliveira, V., Amano, M.T., Correa-Costa, M., Castoldi, A., Felizardo, R.J., de Almeida, D.C., Bassi, E.J., Moraes-Vieira, P.M., Hiyane, M.I., Rodas, A.C., Peron, J.P., Aguiar, C.F., Reis, M.A., Ribeiro, W.R., Valduga, C.J., Curi, R., Vinolo, M.A., Ferreira, C.M. and Câmara, N.O., 2015. Gut bacteria products prevent AKI induced by ischemia-reperfusion. Journal of the American Society of Nephrology 26: 1877-1888. https://doi.org/10.1681/ASN.2014030288
Bellomo, R., Kellum, J.A., Ronco, C., Wald, R., Martensson, J., Maiden, M., Bagshaw, S.M., Glassford, N.J., Lankadeva, Y., Vaara, S.T. and Schneider, A., 2017. Acute kidney injury in sepsis. Intensive Care Medicine 43: 816-828. https://doi.org/10.1007/s00134-017-4755-7
Bowden, J., Davey Smith, G. and Burgess, S., 2015. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. International Journal of Epidemiology 44: 512-525. https://doi.org/10.1093/ije/dyv080
Burgess, S., Dudbridge, F. and Thompson, S.G., 2016. Combining information on multiple instrumental variables in Mendelian randomization: comparison of allele score and summarized data methods. Statistics in Medicine 35: 1880-1906. https://doi.org/10.1002/sim.6835
Capella-Gutiérrez, S., Silla-Martı́nez, J.M. and Gabaldón, T., 2009. trimAl: a tool for automated alignment trimming in large-scale phylogenetic analyses. Bioinformatics 25: 1972-1973. https://doi.org/10.1093/bioinformatics/btp348
Carlier, J.P., Bedora-Faure, M., K’ouas, G., Alauzet, C. and Mory, F., 2010. Proposal to unify Clostridium orbiscindens Winter et al. 1991 and Eubacterium plautii (Séguin 1928) Hofstad and Aasjord 1982, with description of Flavonifractor plautii gen. nov., comb. nov. and reassignment of Bacteroides capillosus to Pseudoflavonifractor capillosus gen. nov., comb. nov. International Journal of Systematic and Evolutionary Microbiology 60(Part 3): 585-590. https://doi.org/10.1099/ijs.0.016725-0
Cheng, X., Wu, B., Liu, Y., Mao, H. and Xing, C., 2017. Incidence and diagnosis of Acute kidney injury in hospitalized adult patients: a retrospective observational study in a tertiary teaching hospital in Southeast China. BMC Nephrology 18: 203. https://doi.org/10.1186/s12882-017-0622-6
Chou, Y.T., Kan, W.C. and Shiao, C.C., 2022. Acute kidney injury and gut dysbiosis: a narrative review focus on pathophysiology and treatment. International Journal of Molecular Sciences 23: 3658. https://doi.org/10.3390/ijms23073658
Davey Smith, G. and Hemani, G., 2014. Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Human Molecular Genetics 23: R89-R98. https://doi.org/10.1093/hmg/ddu328
Emdin, C.A., Khera, A.V. and Kathiresan, S., 2017. Mendelian randomization. JAMA 318: 1925-1926. https://doi.org/10.1001/jama.2017.17219
Er, R.E., Ulusal Okyay, G., Aygencel, B.K.G., Türko Lu, M. and Erten, Y., 2020. Comparison between RIFLE, AKIN and KDIGO: acute kidney injury definition criteria for prediction of in-hospital mortality in critically Ill patients. Iranian Journal of Kidney Diseases 14: 365-372.
Felizardo, R.J.F., de Almeida, D.C., Pereira, R.L., Watanabe, I.K.M., Doimo, N.T.S., Ribeiro, W.R., Cenedeze, M.A., Hiyane, M.I., Amano, M.T., Braga, T.T., Ferreira, C.M., Parmigiani, R.B., Andrade-Oliveira, V., Volpini, R.A., Vinolo, M.A.R., Mariño, E., Robert, R., Mackay, C.R. and Camara, N.O.S., 2019. Gut microbial metabolite butyrate protects against proteinuric kidney disease through epigenetic- and GPR109a-mediated mechanisms. FASEB Journal 33: 11894-11908. https://doi.org/10.1096/fj.201901080R
FinnGen, 2022. FinnGen R7 release. Available at: https://r7.finngen.fi/
Gharaie, S., Lee, K., Newman-Rivera, A.M., Xu, J., Patel, S.K., Gooya, M., Arend, L.J., Raj, D.S., Pluznick, J., Parikh, C., Noel, S. and Rabb, H., 2023. Microbiome modulation after severe acute kidney injury accelerates functional recovery and decreases kidney fibrosis. Kidney International 104: 470-491. https://doi.org/10.1016/j.kint.2023.03.024
Gilbert, J.A., Blaser, M.J., Caporaso, J.G., Jansson, J.K., Lynch, S.V. and Knight, R., 2018. Current understanding of the human microbiome. Nature Medicine 24: 392-400. https://doi.org/10.1038/nm.4517
Gong, J., Noel, S., Pluznick, J.L., Hamad, A.R.A. and Rabb, H., 2019. Gut microbiota-kidney cross-talk in acute kidney injury. Seminars in Nephrology 39: 107-116. https://doi.org/10.1016/j.semnephrol.2018.10.009
Greco, M.F.D., Minelli, C., Sheehan, N.A. and Thompson, J.R., 2015. Detecting pleiotropy in Mendelian randomization studies with summary data and a continuous outcome. Statistics in Medicine 34: 2926-2940. https://doi.org/10.1002/sim.6522
Hartwig, F.P., Davey Smith, G. and Bowden, J., 2017. Robust inference in summary data Mendelian randomization via the zero modal pleiotropy assumption. International Journal of Epidemiology 46: 1985-1998. https://doi.org/10.1093/ije/dyx102
Jang, H.R., Gandolfo, M.T., Ko, G.J., Satpute, S., Racusen, L. and Rabb, H., 2009. Early exposure to germs modifies kidney damage and inflammation after experimental ischemia-reperfusion injury. American journal of physiology. Renal Physiology 297: F1457-F1465. https://doi.org/10.1152/ajprenal.90769.2008
Jia, H., Zheng, Y., Huang, L. and Li, W., 2022. Urinary tissue inhibitor of metalloproteinase-2 and insulin-like growth factor-binding protein 7 enhanced risk prediction for initiation of renal replacement therapy in postoperative patients with acute kidney injury: a prospective cohort study. Journal of Translational Critical Care Medicine 4: 11. https://doi.org/10.4103/JTCCM-D-22-00002
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group, 2012. KDIGO clinical practice guideline for acute kidney injury. Kidney International Supplements 2(1): 1-138.
Kim, C.H. and Moon, S.J., 2021. The role of the gut microbiota in acute kidney injury: a new therapeutic candidate? Kidney Research and Clinical Practice 40: 505-507. https://doi.org/10.23876/j.krcp.21.241
Kobayashi, T., Iwata, Y., Nakade, Y. and Wada, T., 2021. Significance of the gut microbiota in acute kidney injury. Toxins 13: 369. https://doi.org/10.3390/toxins13060369
Kurilshikov, A., Medina-Gomez, C., Bacigalupe, R., Radjabzadeh, D., Wang, J., Demirkan, A., Le Roy, C.I., Raygoza Garay, J.A., Finnicum, C.T., Liu, X., Zhernakova, D.V., Bonder, M.J., Hansen, T.H., Frost, F., Rühlemann, M.C., Turpin, W., Moon, J.Y., Kim, H.N., Lüll, K., Barkan, E., Shah, S.A., Fornage, M., Szopinska-Tokov, J., Wallen, Z.D., Borisevich, D., Agreus, L., Andreasson, A., Bang, C., Bedrani, L., Bell, J.T., Bisgaard, H., Boehnke, M., Boomsma, D.I., Burk, R.D., Claringbould, A., Croitoru, K., Davies, G.E., van Duijn, C.M., Duijts, L., Falony, G., Fu, J., van der Graaf, A., Hansen, T., Homuth, G., Hughes, D.A., Ijzerman, R.G., Jackson, M.A., Jaddoe, V.W.V., Joossens, M., Jørgensen, T., Keszthelyi, D., Knight, R., Laakso, M., Laudes, M., Launer, L.J., Lieb, W., Lusis, A.J., Masclee, A.A.M., Moll, H.A., Mujagic, Z., Qibin, Q., Rothschild, D., Shin, H., Sørensen, S.J., Steves, C.J., Thorsen, J., Timpson, N.J., Tito, R.Y., Vieira-Silva, S., Völker, U., Völzke, H., Võsa, U., Wade, K.H., Walter, S., Watanabe, K., Weiss, S., Weiss, F.U., Weissbrod, O., Westra, H.J., Willemsen, G., Payami, H., Jonkers, D.M.A.E., Arias Vasquez, A., de Geus, E.J.C., Meyer, K.A., Stokholm, J., Segal, E., Org, E., Wijmenga, C., Kim, H.L., Kaplan, R.C., Spector, T.D., Uitterlinden, A.G., Rivadeneira, F., Franke, A., Lerch, M.M., Franke, L., Sanna, S., D’Amato, M., Pedersen, O., Paterson, A.D., Kraaij, R., Raes, J. and Zhernakova, A., 2021. Large-scale association analyses identify host factors influencing human gut microbiome composition. Nature Genetics 53: 156-165. https://doi.org/10.1038/s41588-020-00763-1
Kurki, M.I., Karjalainen, J., Palta, P., Sipilä, T.P., Kristiansson, K., Donner, K. and Nelis, M., 2022. FinnGen: Unique genetic insights from combining isolated population and national health register data. Medrxiv 2022-03. https://doi.org/10.1101/2022.03.03.22271360
LDlink Online Platform, 2023. Available at: https://ldlink.nci.nih.gov/
Lee, K.S., Jeong, Y.J. and Lee, M.S., 2021. Escherichia coli Shiga Toxins and gut microbiota interactions. Toxins 13: 416. https://doi.org/10.3390/toxins13060416
Li, N.N., Kang, K., Zhou, Y., Liu, Y.Q., Zhang, Q.Q., Luo, P.Y., Wang, L., Man, M.Y., Lv, J.F., Wang, X.B., Peng, Y.H., Luan, F.Y., Li, Y., Zhang, J.N., Chong, Y., Wang, Y.Q., Wang, C.S., Zhao, M.Y. and Yu, K.J., 2024. Throat microbiota drives alterations in pulmonary alveolar microbiota in patients with septic ARDS. Virulence 15: 2350775. https://doi.org/10.1080/21505594.2024.2350775
Liu, X., Mo, J., Yang, X., Peng, L., Zeng, Y., Zheng, Y. and Song, G., 2024. Causal relationship between gut microbiota and chronic renal failure: a two-sample Mendelian randomization study. Frontiers in Microbiology 15: 1356478. https://doi.org/10.3389/fmicb.2024.1356478
Luo, S., Zhao, Y., Zhu, S., Liu, L., Cheng, K., Ye, B., Han, Y., Fan, J. and Xia, M., 2023. Flavonifractor plautii protects against elevated arterial stiffness. Circulation Research 132: 167-181. https://doi.org/10.1161/CIRCRESAHA.122.321975
Machado, R.A., Constantino de S., L., Tomasi, C.D., Rojas, H.A., Vuolo, F.S., Vitto, M.F., Cesconetto, P.A., de Souza, C.T., Ritter, C. and Dal-Pizzol, F., 2012. Sodium butyrate decreases the activation of NF-κB reducing inflammation and oxidative damage in the kidney of rats subjected to contrast-induced nephropathy. Nephrology, Dialysis, Transplantation 27: 3136-3140. https://doi.org/10.1093/ndt/gfr807
MiBioGen Consortium, 2022. MiBioGen. Available at: https://mibiogen.gcc.rug.nl/
Mikami, A., Ogita, T., Namai, F., Shigemori, S., Sato, T. and Shimosato, T., 2021. Oral administration of Flavonifractor plautii, a bacteria increased with green tea consumption, promotes recovery from acute colitis in mice via suppression of IL-17. Frontiers in Nutrition 7: 610946. https://doi.org/10.3389/fnut.2020.610946
Monard, C., Meersch-Dini, M. and Joannidis, M., 2023. When the kidneys hurt, the other organs suffer. Intensive Care Medicine 49: 233-236. https://doi.org/10.1007/s00134-022-06925-5
Nguyen, L.T., Schmidt, H.A., von Haeseler, A. and Minh, B.Q., 2015. IQ-TREE: a fast and effective stochastic algorithm for estimating maximum-likelihood phylogenies. Molecular Biology and Evolution 32: 268-274. https://doi.org/10.1093/molbev/msu300
Ogita, T., Yamamoto, Y., Mikami, A., Shigemori, S., Sato, T. and Shimosato, T., 2020. Oral Administration of Flavonifractor plautii strongly suppresses Th2 immune responses in mice. Frontiers in Immunology 11: 379. https://doi.org/10.3389/fimmu.2020.00379
PhenoScanner GWAS Database, nd. Available at: http://www.phenoscanner.medschl.cam.ac.uk/
Pruesse, E., Peplies, J. and Glöckner, F.O., 2012. SINA: accurate high-throughput multiple sequence alignment of ribosomal RNA genes. Bioinformatics 28: 1823-1829. https://doi.org/10.1093/bioinformatics/bts252
Ronco, C., Bellomo, R. and Kellum, J.A., 2019. Acute kidney injury. The Lancet 394: 1949-1964. https://doi.org/10.1016/S0140-6736(19)32563-2
Saranya, G.R. and Viswanathan, P., 2023. Gut microbiota dysbiosis in AKI to CKD transition. Biomedicine and Pharmacotherapy 161: 114447. https://doi.org/10.1016/j.biopha.2023.114447
Singer, M., Deutschman, C.S., Seymour, C.W., Shankar-Hari, M., Annane, D., Bauer, M., Bellomo, R., Bernard, G.R., Chiche, J.D., Coopersmith, C.M., Hotchkiss, R.S., Levy, M.M., Marshall, J.C., Martin, G.S., Opal, S.M., Rubenfeld, G.D., van der Poll, T., Vincent, J.L. and Angus, D.C., 2016. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 315: 801-810. https://doi.org/10.1001/jama.2016.0287
Staiger, D., 1997. Instrumental variables regression with weak instruments. Econometrica 65: 557-586.
Verbanck, M., Chen, C.Y., Neale, B. and Do, R., 2018. Publisher correction: detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nature Genetics 50: 1196. https://doi.org/10.1038/s41588-018-0164-2
Wang, H.E., Muntner, P., Chertow, G.M. and Warnock, D.G., 2012. Acute kidney injury and mortality in hospitalized patients. American Journal of Nephrology 35: 349-355. https://doi.org/10.1159/000337487
Yu, H., Wan, X., Yang, M., Xie, J., Xu, K., Wang, J., Wang, G. and Xu, P., 2023. A large-scale causal analysis of gut microbiota and delirium: a Mendelian randomization study. Journal of Affective Disorders 329: 64-71. https://doi.org/10.1016/j.jad.2023.02.078
Yu, K.J., 2022. Timing for initiating renal replacement therapy in patients with acute kidney injury: Late is better? Journal of Translational Critical Care Medicine 4: 2. https://doi.org/10.4103/JTCCM-D-21-00025
Zhu, H., Cao, C., Wu, Z., Zhang, H., Sun, Z., Wang, M., Xu, H., Zhao, Z., Wang, Y., Pei, G., Yang, Q., Zhu, F., Yang, J., Deng, X., Hong, Y., Li, Y., Sun, J., Zhu, F., Shi, M., Qian, K. and Zeng, R., 2021. The probiotic L. casei Zhang slows the progression of acute and chronic kidney disease. Cell Metabolism 33: 1926-1942.e8. https://doi.org/10.1016/j.cmet.2021.06.014




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}