æè¦
Abstract
The concept of jing is fundamental in Chinese medicine (CM). However, English-language discourse reveals the term to be polysemous, confusing, and contradictory. In the currently flourishing field of Chinese reproductive medicine in the West, clinicians claim to be able to provide treatment for age-related pathologies of the human gametesâascribed by modern CM to be manifestations of jingâthat seem dubious from the perspective of modern biomedicine. Such practitioners reveal scripts that diverge significantly from their biomedical peers. In the context of the unclear modes in which the concept of jing functions, and the emotive sphere of reproductive medicine in which it operates, this paper uses a grounded theory approach to make a thematic analysis of the relevant English-language discourse relating to jing. Interpretive analysis of the resulting themes shows the term being used differently by clinicians and scholars of CM, and that such modes are predicated according to the specific requirements and agendas of the author. Finally, recommendations for clinicians, scholars, and researchers are made along with concluding remarks.
Introduction
The concept of jing (ç²¾, usually translated as âessenceâ, but left in the Chinese here to allow the term semiotic freedom), is fundamental in CM. Standard core texts used in modern CM education in the West1 tend to present jing as part of an established, ahistorical, and internally congruent theoretical framework, in which it constitutes the material foundation of a hierarchy of increasingly subtle and immaterial âvital substancesâ that form the building blocks of CM physiology. However, such systematisation flies in the face of scholarship showing CM to be heterogenous and in constant transformation.2 The apparently well-ordered system into which the concept of jing is inserted is far from universal, and authors who look more deeply into the concept find paradox and multiplicity of meaning;3 Zhang and Rose, for example, list 22 meanings inherent in the term.4 The concept of jing is theoretically problematic: for example, jing is commonly said to be irreplaceable,5 and yet many CM texts list âjing deficiencyâ as a pattern differentiation for specific diseases6âespecially reproductive dysfunction7âand provide acupuncture points8 and herbs9 that can treat such a disharmony.
When looked at through the prism of reproductive medicine, further questions arise. In the flourishing field of CM fertility treatment in the West,10 clinicians posit that CM treatment can enhance fertility by improving âegg qualityâ,11 sperm count and quality,12 and even turn back the âreproductive clockâ of women whose egg supply isâbased on laboratory testsâexhausted.13 Such clinical results seem unlikely from the perspective of modern biomedicine, which asserts that women are born with all the eggs they will ever have, that gradually decline in quality with age, and that once used up are gone forever.14 One might question exactly what CM clinicians mean by improving âegg qualityââwhether enhancing the general cellular vitality of the gametes or even changing their genetic make-upâand how such claims relate to traditional CM theory. Perhaps there are indeed subtle physiogical variablesâas yet undiscovered by Western medicineâthat can be influenced by CM to enhance fertility? Or perhaps the expediency of market forces is leading practitioners to trade on the Oriental mystery that surrounds CM in the West to make unrealistic claims of its clinical potential? Or perhaps naïve Western clinicians are simply reading superlativeâbut ultimately unrealisticâpossibilities into CM theory that were not intended by its authors.
Given that modern biomedical treatment is able to control virtually all aspects of fertility other than the overall quantity and quality of the gametes themselves, practitioners of complementary medicine who claim to be able to influence these factors will be highly sought after by potentially vulnerableâand frequently desperateâpatients.15 The public discourse of such practitioners tends to reject standard biomedical scripts regarding the arbitrary limitations signified by laboratory tests, and instead presents a message of hope backed by a mixture of Chinese and biomedical theory together with unsubstantiated case studies of ageing patients who were able to conceive against the odds with the help of CM.16 Given that practitioners of complementary medicine are frequently accused of providing false hope to patients,17 it would seem apposite to examine this area of CM to find out how the concept of jing is operating.
After presenting the methodology and literature search for this research, a basic orientation is provided that documents a standard modern reading of jing. Then the main themes are described, followed by detailed discussion before concluding comments are made. It should be pointed out that this paper has significant limitations. The author is a Western practitioner of CM who does not read Chinese and this paper is a study of modern English-language texts written primarily by Western authors. As such any conclusions pertain only to such modern Western discourse, and does not purport to offer a valid assessment of historical Chinese sources.
Methodology
This paper uses a grounded theory approach18 to conduct a thematic analysis of the relevant English-language sources. Thematic analysis is a highly inductive method that facilitates identification, analysis, and interpretation of patterns within data19 in order to allow new theories and interpretations to emerge.20 It is an inherently flexible method and can be applied across a range of theoretical and epistemological frameworks, and as such is ideally suited for the novice researcher.21 In the case of this paper, the relevant data was first identified through a systematic literature search, after which sensitive reading and re-reading of the texts was conducted whilst applying coding to the relevant sections.22 The resulting codes were then inductively developed into themes using a reflexive process that involved repeated revisiting of the data and comparison between the different codes and themes.23 During this process the following hypothesis emerged from the data: The concept of jing in English-language texts is polysemous, contradictory, and confusing, and there is a lack of congruence between its presentation in the extant historical literature and how it is used in the modern clinical practice of CM.
The identified themes were analysed using an interpretive approach, before being summarised into concluding theories. The epistemological perspective employed is essentially that of social constructivism, which presupposes that CM wasâand continues to beâcollectively invented and reinvented by various groups at different times.24
Literature search
An online search was made of the following electronic databases:
PubMed
AMED
MEDLINE
AltHealthWatch
In order to avoid using an unwieldy search algorithm, two separate search algorithms were used as follows:
â(jing OR essence) AND (Chinese medicine)â: to elicit articles that discuss the concept of jing directly.
â(Chinese medicine OR TCM) AND (fertility OR infertility OR reproduct*) AND (sperm OR egg OR ooctye OR ovarian reserve OR premature ovarian failure OR oligospermia OR aspermia OR azoospermia)â: to identify papers that discuss the treatment of reproductive disorders associated with the concept of jing.
The searches returned a total of 825 articles. These were initially filtered by title and abstract to exclude irrelevant articles, duplicates, and incorrectly indexed articles. Articles were included where they:
Directly discussed the CM concept of jing.
Studied reproductive medicine with reference to the CM concept of jing or other related CM concepts (such as the Kidney) or biomedical subjects (such as gametes or genetic factors).
Contributed to the discourse on jing in other ways by exploring issues of Chinese reproductive medicine, translation, or history.
The sifting process resulted in a total of 18 articles. Additional relevant studies were sought in the reference lists of identified papers, and by searching the online Chinese medicine journals and databases. In order to identify relevant books, an online search was made of the catalogue of the British Libraryâs catalogue; further texts were identified in the bibliographies of these texts, and by manually searching the library of the University of Westminster (London, UK). In addition, in order to examine the discourse around jing in the public domain, an internet search was made using various combinations of the terms âjingâ, âessenceâ, âgametesâ, âovarian reserveâ, âspermâ, and âChinese medicineâ.
The resulting data were found to fit into the following categories:
Clinical research into the CM treatment of reproductive disease, for example, premature ovarian failure, azoospermia, etc.
Cultural/sociological/historical discussions of Chinese reproductive medicine.
Core texts on Chinese medical theory or Chinese reproductive medicine.
Public-facing websites providing information for potential patients of Chinese reproductive medicine.
A full description of the above search methodology can be found in Appendix 1.
Basic orientation
The Chinese character for jing, ç²¾, is made up of the significant component mi, meaning rice or kernel of grain, and the phonetic component qing, which signifies the colour of lush and vibrant growth and which is thought to contribute to the characterâs meaning.25 Given the supreme importance of rice throughout Chinese history, the image of a lush green rice sprout issuing forth from seed is a culturally compelling symbol of the generative power of life. A typical CM taxonomy involves jing being divided into three types: pre-heaven (or âinnateââsaid to be formed at conception from the coalescing of the essences of the parents), post-heaven (or âacquiredââthe product of metabolism from eating and breathing), and Kidney jing (which governs growth, development, sexual maturation, reproduction, and pregnancy).26 As well as its more abstract meanings, jing also has the narrow meaning of semen.27 It should be noted here that, given the focus of this paper on reproductive medicine, the emphasis will be on what is referred to above as âKidney jingâ. Unfortunately it is beyond the scope of this paper to explore the extensive historical discourse discussing the closely-related doctrines of Mingmen (âlife gateâ), the Kidneys, and the chong and ren vessels.28
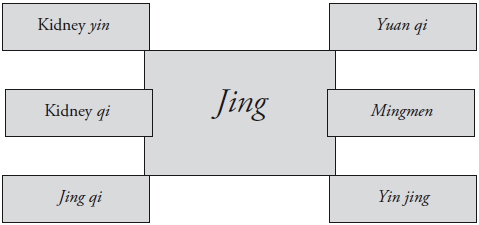
Beyond standardised modern readings of jing, close reading of the literature reveals a tangled web of terms with overlapping meanings and shifting signification. The sample of texts surveyed here reveals a variety of terms, all of which express some aspect of the concept of jing : âyin essenceâ, âyang essenceâ, and âKidney-qi essenceâ;29 âyin jingâ;30 âjing qiâ;31 yuan (primal) qi;32 and âkidney qiâ.33 For Ross, jing is a âgroup of overlapping conceptsâ,34 and the term is also frequently used in the plural âessencesâ;35 indeed, Dharmananda documents its use to describe any dense physiological fluids (for example, saliva, breast milk, vaginal fluids, etc.).36 Even where standardisation and semantic clarity is the primary focus of a text, jing seems to elude simple definition.37
Themes
The following ten themes were identified:

Various CM terms overlapping with the concept of jing.
Citation: Asian Medicine 7, 2 (2012) ; 10.1163/15734218-12341260
Gametes
A primary theme in the literature is that of jing being used as a direct analogue with the biomedical concept of the gametes. For example, Lyttletonâarguably the most influential Western authority on the CM treatment of infertility and a self-professed exponent of Chinese and Western medicine âfusionââboldly states that âwhat the doctors in China 2000 years ago were referring to when they described the Kidney Jing is what modern Western medical science refers to as the gametes or eggs and sperm themselves.â38 In such a reading of jing, a pattern of jing deficiency corresponds to a pathological lack of eggs or spermâpremature ovarian failure or azoospermia, for exampleâfor which a viable clinical strategy is to âstrongly reinforce the Kidney Jing to try and influence the nature of the eggs themselvesâ.39 Whilst appealing in its simplicity and pragmatism, the idea of the narrow correspondence between jing and the gametes is not universal. For example, a modern paper discussing Chinese herbal medicine (CHM) and egg quality does not refer to jing at all.40 Clearly, it is not a clinically indispensable concept, even when egg quality and quantity are the primary focus.
Menstrual blood
Prior to the twentieth century, practitioners of CM did not know about eggs or sperm, but rather the female analogue to male jing (semen) was menstrual blood. Traditional doctors were aware that when a woman became pregnant, menstruation ceased, and thus deducedâerroneously as we now knowâthat conception was the result of the coalescing of the male semen and female blood. Unschuld quotes the sixteenth-century author Zhang Huang, âMan has life because he . . . has received from his father and mother semen and blood. When [the latter two] contact each other, they unite and congeal to become a fetus in the womb.â41 The Qing-dynasty gynaecological expert Fu Qingzhu further explains that âMenstruation is not blood but heavenly water or the tian gui. Originating in the kidneys, it is the essence of consummate yin . . . it is red like blood, but it is, in fact, not blood. . . . People nowadays regard the menstrual flow as blood, but this is an incorrect assumptionâ.42 Such a belief is frequently encapsulated in the pithy phrase âMenstruation comes from the Kidneyâ,43 although modern readings take this to mean that the Kidney governs the hormonal functions of the hypothalamic-pituitary-ovarian axis.44 Because jing was traditionally viewed as extremely precious, menstruation was viewed as severely depleting,45 such that Daoist nuns would practise specific qigong exercises in order to stop menstruation and thus preserve their jing.46 Regulation of the menstrual cycle was thus of primary importance in traditional womenâs medicine and seen to have effects far beyond merely reproductive function.47 Congruent with this, published cases of infertility tend to show pregnancy occurring as soon as the menstrual cycle has been sufficiently regulated.48 However, the view of menstrual blood as a precious manifestation of jing conflicts with other widely-held Chinese folk beliefs that menstrual blood is a superfluous and unclean pollutant,49 suggesting that competing scripts have been active through Chinese history.
DNA and heredity
Modern authors frequently make a direct correspondence between jing and DNA. For example, in cases of male infertility due to chromosomal abnormality, Lyttleton identifies the causative factor as âKidney Jing weaknessâ.50 Such a correspondence is perhaps unsurprising, given that the typical characteristics of jingââderived from the parents . . . provides for a personâs constitutional make-up . . . a fixed substance that cannot be added to or replenished.â51âcould be just as accurately applied to DNA. Such correspondence is frequently made without acknowledging any semantic or cultural complications: thus for Magidoff âmutated DNAâ is âchanges in the jingâ.52 Damone, on the other hand, exhibits more paradigmatic sensitivity by describing reproductive essence as âgenetic-likeâ.53 Whilst a general thread runs through the literature acknowledging the difficulty of altering the genetic make-up of gametes with CM, a recent study suggests that this may in fact be possible with CHM.54 Horne argues that the possible mechanism of this may involve influencing epigenetic components that dictate how genes are expressed throughout the reproductive system.55
Developmental stages
The locus classicus of jing and reproductive theory is undoubtedly the first chapter of the Huang Di Nei Jing Su Wen, in which the seven- and eight-year cycles of females and males are described (see Appendix 2). The âTian guiâ (also translated as âKidney waterâ, or the more opaque âHeavenly Tenthâ by Wiseman and Feng56) referred to in this chapter is widely understood to refer to jing âin its role in creating the menstruateâ,57 and is frequently glossed without the semantically difficult âtian guiâ (âessence is responsible for the onset of puberty, fertility and the menopauseâ).58 Thus tian gui describes an essentially temporal process that, where pathological, can be treated via the jing, âIf periods never begin (primary amenorrhoea) . . . the TCM doctor will treat the Kidney Jing.â59 It is noteworthy that in CM the arrival of tian gui is seen to be a virtually identical process in males and females (with minor differences in timing60), whereas in biomedicine, puberty and the ending of reproductive capacity are governed by fundamentally different physiology. Thus oogenesis begins in females before they are born and continues until âthe pool of remaining ovarian follicles becomes exhaustedâ in their forties, whilst spermatogenesis starts in males at puberty and âhealthy men . . . can retain reproductive capacity into their eighties or ninetiesâ.61 Such differences call into question the direct commensurability of jing with such biomedical analogues.
Matter and spirit
Unlike most CM concepts that tend to be processual in focus,62 jing easily becomes glossed as a static material form. This probably originates from the the Su Wen statement, âEssence is the root of the human body.â63 A modern Chinese textbook subtly distorts this into the more decisively earthbound, âessence is the material base of the human bodyâ64. For Sivin, jing is a âfundamental substanceâ, for Porkert, it is âthe concrete basis of . . . individual existenceâ, Damone describes it as a âraw materialâ and for Kaptchuk, it is a âtextureâ.65 Thus jing is frequently portrayed as a kind of anabolically-potent source material from which semen, blood, bone marrow, brain, and spinal cord originate, and as such represents the earthly base of a continuum of increasingly subtle physiology that culminates in shen. Such a model matches agreeably for modern sensibilities with scientific distinctions of solid, liquid, and gas (represented by jing, qi, and shen).
However, the conceptual borders of jing are not always so distinct. Although associated with the physical body, Larre and Rochat de la Vallée suggest that âEssences have no form and no shape. They are the condition of any shape, they are able to make any and every formâ.66 Damone presents the beguiling theory in this regard that jing represents the stem cells from which all other physical substance and cells are derived.67 There are clearly dynamic potentials within jing; as Larre and Rochat de la Vallée state, âEssences are . . . the elements or components of life, and life is inside these componentsâ.68 Horne makes a cogent point of comparison in relation to gametes, which are not inert lumps of cytoplasm (i.e., yin without yang), but are filled with thousands of times more mitochondria than typical human cells69âtiny energy factories which have been found to respond to CHM.70 In CM it is of course impossible to have yin physical substance independent of yang: âQi can generate essence, and essence can generate Qi.â71 Porkertâs âstructive potentialâ is illuminating in this regardâwhere âstructiveâ is a complement to the âactiveâ principle represented by qi and shen, and implies the capacity âto render concrete, to substantiate, a given effect without regard to its qualityâ.72 Such a reading harks back to chapter eight of the Ling Shu that states, âThe kidney stores essence; essence is the abode of spiritâ. This relationship is repeated in chapter 36 of the Nan Jing, where jing is first introduced as the dyad âspirit-essenceâ (see Appendix 2). To forget the âverticalâ interpenetration of jing with shenâwhich modern reductive readings of the term seem toâcan have repercussions with regard to fertility treatment, âA change on the shen level also involves a change on the jing level . . . in this sense shen facilitates fertility on the physical level.â73 To this end, modern clinicians of CM frequently emphasise psychoemotional support in their treatment programmes for poor ovarian reserve.74
Quantity and decline
The theme of jing being material in nature is closely associated with it being presented as being restricted in quantity and undergoing continuous declineâsomething like a candle burning inexorably down. Indeed, Dharmanda documents the traditional Chinese fears around declining jing recorded in a Ming Dynasty novel that tells the story of a man who dies from sexual indulgence, whose doctorâs concluding comment is âThe candle flickers once the oil is used upâ.75 Thus Flaws states: âWe are each endowed with a certain quantity and quality of this . . . at the moment of conception and this cannot be augmented or modified.â76 It is a âfinite bundleâ77 that is either plentiful or scantâsuch that Lyttleton is able to divide its pathological lack into severe, moderate; and mild, each with specific symptoms.78 The view that jing (as eggs) âgets used up with the hundreds of menstrual cycles a woman experiencesâ79 is mirrored by biomedicineâs precise numerical formulations: âat birth, approximately 200,000 to 2,000,000 primary oocytes remain in each ovary . . . and around 400 will mature and ovulate during a womenâs reproductive lifetimeâ.80 Such temporal diminution of the gametes is also the case for men, âsperm production decreases 50â70% between ages 60 and 80â.81 The Chinese notion that men lose jing through ejaculation is associated with a long tradition extolling the benefits of sexual abstinence,82 so that Chinese doctors frequently advise sexual abstinence in cases of infertility.83 Originally it was thought that just excessive sexual activity depleted the jing, but the Qing dynasty doctor Wu Tang (1758â1836) expanded this so that âall human activity can agitate and disturb the essenceâ.84 However, although such linear temporal decline tallies nicely with the biomedical view of the gametes, it is at odds with the theory that jing is continually augmented by postnatal jing (and thus jing operates metaphorically more like a rechargeable battery than a candle).
Whilst primarily quantitative in nature, discourse on the decline of jing sometimes involves qualitative entropy that is often likened to the damage suffered by DNA in Western theories of reproductive ageing.85 Thus Lyttleton reports that âless than ideal Jing may be inherited if the parents are older than 40â.86 Lyttleton criticises Western artificial reproductive technology (ART) for pursuing quantity at the expense of quality, âKidney Jing, that hard-to-measure quality of inheritance, is being ignoredâ. Indeed, ART seems to produce male offspring who themselves have compromised reproductive health.87 Such understandings have a historical basis in traditional CMâas Wu documents, traditional doctors would blame anomalies, such as hermaphrodite offspring, on the jing.88
The clinical utility of the concept of jing ultimately rests on whether clinicians are able to intervene if it is found to be deficient. One of the difficulties in assessing this is that authors tend to present only successful case studies. Liang, for example, documents a 48-year-old perimenopausal woman who, after CM treatment, managed to produce 18 eggs during an IVF cycle and successfully conceive.89 Lewis90 and Horne91 also describe cases where women in their late forties were able to conceive with help from CM. For many authors, jing deficiency is an entirely relevant clinical distinction and âtonify jingâ a viable treatment strategy.92 For example, Jin gives âExcessive consumption of Kidney Essenceâ as a pattern differentiation for oligospermia, and provides his own formulaââJinâs decoction for replenishing essence and sperma liquefaction to nourish the Kidney and replenish Kidney essenceâ.93 Lyttleton acknowledges that treatment of jing deficiency requires long-term treatment (over months and years), and asserts her experience of doctors in China providing successful treatment in cases of jing deficiency.94 Indeed, numerous clinicians explicitly assert that CM is able to improve egg quality in cases where biomedicine is unable to help.95
Lewis, a high-profile CM reproductive specialist, is at pains to reject typical Western ideas of reproductive ageing and presents her perspective on âthe truth about our eggsâ, in which âthe ocean of our fertility doesnât dry up; it just becomes still. And with help it can flow once more.â96 She tends to side step the idea that the body âruns outâ of something (jing/eggs), and instead posits the decline in fertility due to age as being due to âhormonal balance and blood flowâ.97 It may be that such a view has a historical basis in traditional CMâas Farquhar suggests, âthe discrete transplantable objects of Western medicine . . . are seen as mere products of powerful processes that govern the life of the body.â98 Lewis also disputes the effects of ageing on egg quality: âcontrary to what Western medicine would lead us to believe, a womanâs eggs do not have an âexpiration dateââ.99 Anecdotal evidence seems to confirm that CHM may indeed be able to restore reproductive capacity, even in relatively severe cases of premature ovarian failure.100 Horne boldly supports such a notion (âWe can reverse signs of aging until a woman enters the menopauseâ), and provides treatment protocols that involve âslowing or reversing oocyte agingâ.101 Such protocols might be seen to be supported by Chinaâs long historical tradition of practices designed to prevent or replace the loss of jing, especially from within the Daoist tradition.102
Other authors are more careful to avoid the emotionally charged issue of âturning back the clockâ with regard to reproductive capacity. Elliott, for instance, disputes that CM treatment can prevent the affects of ageing on egg quality.103 West, a high-profile infertility specialist in the UK, asserts her awareness âthat a woman is born with all the eggs she is ever going to haveâ but maintains that âyou can improve the environment that the existing eggs are growing inâ by using acupuncture to âhelp improve blood flow to the ovaries, as this reduces significantly with ageâ.104 Heese initially asserts that CM cannot turn back time and affect egg quality, but is later apparently unable to resist an about-face: âWhilst it cannot turn back time and improve egg quality in an older woman, it may . . . indirectly influence its maturity and quality.â105 Most authors seem to side-step the contradiction inherent in CM theoryâthat the gradual depletion of jing is a natural part of ageing but as soon as it becomes a barrier to conceiving it is made pathological. Liang, however, acknowledges this, stating that âAlthough this [decline] is a natural stage of a womanâs development, for the purposes of achieving pregnancy, it is considered a pathology hereâ.106
Yin and fluids
Jing is widely associated with yin and fluids: âQi belongs to Yang whereas blood and essence belong to Yinâ.107 Hammer clinically tangible evidence supporting this theory: âKidney essence is often associated more with Kidney yin than with Kidney yang; partially because on the pulse, deficiency of Kidney yin and Kidney essence have similar qualities (tight and wiry).â108 Lin and Flaws suggest a broader classification, in which âyin jingâ includes jing, blood, and jin yeâall of the fluid aspects of the body.109 Elsewhere, however, Flaws equates jing directly with Kidney yin: âKidney yin is the jing essence and the substantial aspect of the kidney.â110 Other authors, however, point out that jing can be seen to be âbeforeâ yin and yangâand thus the origin of both.111 For some authors, female sexual secretions are manifestions of jing,112 whilst Lyttleton disputes this based on the narrow equation of jing with gametes: âSince these secretions do not contain gametes, they do not have such a direct connection to the Jing. Rather, they reflect Kidney Yin reserves.â113 Historically, some doctors have taken the idea of jing being a fluid-like material substance to its logical conclusion, leading to various historical arguments regarding the topography of literal âpathways of essenceâ connecting the brain, Kidneys, and reproductive organs.114 As a sidenote, the herbs that tonify jing in the material medica tend to be warm, sweet, and salty yang tonics, rather than the moist, cool, and sweet medicinals that one might expect to support yin and fluids.115
Reproductive strength and constitution
In CM terms strong jing implies a dyad of robust constitution combined with a high reproductive capacity at both macro and micro levels, so that Lyttleton states that âPlentiful Jing increases fertility . . . women who are successful in having babies in their 40s . . . often live longer than averageâ116 and âsperm that lack the wherewithal to carry out penetration and fertilisation of egg cells [reflect] quite serious Kidney Jing deficiency.â Wu details that such reproductive strength was traditionally viewed as being intrinsic in the jing itself, such that where male jing dominated it would produce a boy and vice versa.117 However, the linear equation âmore jing=greater reproductive potentialâ might be seen to be challenged by modern studies in which increased frequency of ejaculation actually improves sperm quality and quantity.118
Sex and morality
Because jing is inseparable from reproductionâand therefore sexâtraditional Chinese discourse around it unsurprisingly reveals moral scripts. The origins of such sensitivities might be traced back to the Su Wen, where Qi Bo explains that, âThe people of today . . . through their lust they exhaust their essence, through their wastefulness they dissipate their true [qi].â119 In a commentary by Wang Bing, he elucidates: âTo make frivolous use [of oneâs essence] is called âwastefulness.â . . . it is because the sages cherished [their] essence and carefully considered its use that their bones were full of marrow and strong.â120 Thus jing is used as moral currency to make a point about physically weakening effects of licentiousness sex. Such scripts continue to the present dayâfor Xingzhe âSex is worse than tigers or wolvesâ and âanything that excites desire, especially sexual desire, disturbs jing . . . unbridled craving for things is ultimately weakening for the whole society; less essence, less spirit, less will.â121 Both quotations reveal a discourse in which jing is the link between frivolous sex and a weakening of the very foundations of the individual body and society. In the case of women, Furth has clearly documented how the depleting effects of female gestational functions were associated with a discourse that emphasised womenâs fundamental weakness in comparison to men.122 Further gendered questions might be asked about how the label for the male seed became synonymous with the generative aspect of life in a patriarchal society.123
Depth and density
Discourse around jing frequently emphasises qualities of depth and density: âthere is a kind of earthly aspect, a density. . . . Essences are very dense because they are full of life;124 âit is the life spring sourced in our deepest origins . . . [if] the deficiency is deep, treatment needs to be strong, persistent, and lengthyâ.125 This is epitomised in the nature of semen, âsperm. . . . In the form of a liquid it is nothing other than a very rich and dense possibility of making lifeâ.126 Treatment of jing is usually through herbs (rather than acupuncture), in particular herbs thatâaccording to the Nei Jingâhave âaffinity for flesh and bloodââe.g., animal products. Given that in western countries, such as the UK, animal products are banned, one might question whether it is possible to tonify jing effectively with the remaining available CHMs. Damone quotes Ye Tianshi (1667â1746) in this regard: âEssence and blood have form. [Therefore do not] use grasses and woodâsubstances, which lack feeling. . . . Their qi does not correspond to [essence and blood]â.127 Unsurprisingly, given its multiple identities, a variety of words express the effects of herbs on jing. Thus Shan Yao and Tu Si Zi âsecureâ jing, Don Chong Xia Cao and Ba Ji Tian âaugmentâ jing, Shu Di Huang and Lu Rong âgenerateâ jing, Zhi He Shou Wu âpreservesâ jing, E Jiao âreplenishes Kidneyâ jing, Rou Cong Rong âenrichesâ jing and Bu Gu Zhi âstabilisesâ jing.128 Because Kidney jing is nourished by post-heaven jing, clinicians working in the area of low egg reserve tend to make diet and nutrition a high priority,129 frequently employing substances from modern naturopathic nutrition such as wheatgrass, royal jelly, Co-Enzyme Q-10,130 algae, and seaweed.131 Arguably the quintessential substance to tonify jing is Zi He Che (Hominis Placenta), which according to the Commentary on the Divine Husbandmanâs Classic of Materia Medica, âtonifies dual deficiency of yin and yang, with the ability to restore the root and return the primal [qi]â.132 Assessing the constituents of this substance from a biomedical perspective is revealing, and reads like a primitive combination ART medicineâcomplete with gonadotropins, estradiol, progesterone, and prolactinâto powerfully activate the endocrine glands.
Discussion
Historicising jing
Modern Western clinical texts frequently present CM as an ahistorical system that was defined millennia ago and has endured without change.133 Recent scholarship, however, suggests that CM is âdeeply historicalâ,134 and documents the complexities of its relationship with modern biomedicine.135 Modern Chinese reproductive specialists areâby definitionâpractitioners of âintegrated Chinese-Western medicineâ,136 and as such represent the fruit of the Communist agenda of integration and âscientisationâ.137 Liang, for example, epitomises the typical mindset of the modern CM gynaecologist when she states that, âThe Chinese medical concept of the kidneys correspond directly to the endocrine and reproductive systemsâ138 (and congruent with such a view Liang supplements the Kidneys in virtually all of her case studies of ageing women). Li similarly elevates the Kidney to a physiological position in andrology: âOnly the kidney is the crucial organ for male infertility . . . insufficient essence is the fundamental causative factor of male infertilityâ.139 Modern Western âspecialistsâ in the field of Chinese reproductive medicine, of course, learnt their trade since biomedicine arrived so forcefully in China, and unsurprisingly therefore tend to stick close to the modern âparty lineâ of integration, such that CM concepts and theory remain congruent with biomedicine.140
At some point during the twentieth century, CM had to grapple with the reality of eggs and sperm (first discovered by the seventeenth-century European biologist Leeuwenhoek)141âand the derision from some quarters that it did not know about them.142 Farquhar has documented the pressure exerted on CM during the late twentieth century to come up with similar tangible entities to those recently discovered by biomedicine (e.g., bacteria, viruses, gametes, etc.).143 Fortunately, representatives of CM were able to save face by pointing out the correspondence of the gametes with jing, simultaneously proving that CM was way ahead of its time. As a happy coincidence, polarising the focus of conception around jing (and thus the Kidneys) meant that the potentially humiliating theory that semen unites with female blood at conception could be allowed to fade into obscurity.
It is of course not an entirely modern occurrence to gloss jing as a physical object (whether âthe bodyâ or âgametesâ)âthis has a historical basis in its alternative identity as semen. Whilst it is impossible to verify how the pre-Han originators of CM conceived of jing, one might imagine that despite their primary focus on process, resonance, and relationship,144 they still had to somehow classify the physical âstuff â of the human bodyâphysicality that visibly suffered inexorable temporal decline, with an associated deterioration in reproductive capacity. It may be that jing fitted as a descriptor of the âbodyâ in this regard.
For modern clinicians, who tend to tread a path somewhere between CM and biomedicine, considering jing as âthe refined part of all the qi in the universe [and] all the useful entities within the human bodyâ eludes clinical utility.145 Practitioners are required to make clinical decisions, and jing is therefore required to take on the identity of a physical substance that can be present or deficient in discrete amounts and thereby influenced through treatment. Such narrow readings, however, exhibit the common tendency to edit out the contradictions and anomalies that do not fit oneâs own agenda when assembling a coherent version of another cultureâs medicine.146 Thus for modern clinicians the scope of jing identified in the themes aboveâthat includes aspects of form, function, and processâbecomes restricted in the interests of clinical expediency.
Historians and philosophers, on the other hand, tend to allow jing a broader scope of meaning, asserting that to conceive of it as a fixed physical entity is anathaema to CM, as jing is by definition in a process of continuous movement and transformation.147 For a medicine that assumes âtransformation as the inalterable condition of being . . .â Farquhar argues, â. . . essences that are permanent . . . are not issues for discourseâ.148 Just as clinicians require jing to assume an identity with which they can work, it is the job of the scholars to allow the manifold meanings of jing to shine. Historians and philosophers, of course, invariably read classical Chinese, and thus may be able to embrace multiple semantic subtleties, whilst modern clinicians may have to settle for the meaning appropriate to the matter at handâin the case of reproductive medicine, the gametes (although it should be noted that modern Chinese practitioners seem to share equally narrow readings of the term). However, Wu argues against the tendency of scholars to disproportionably privilege CM medical scripts of function (âvital flows and transformationâ) over form (âthe physical bodily spaceâ), identifying both as forming a vital tension in the discourse of traditional doctors of CM.149
That the term jing defies straightforward linguistic capture in English should come as no surprise. Translation of CM is highly problematic150 as there is invariably no one-to-one correspondence between English and Chinese words151 and Chinese meaning tends to operate contextually.152 Add to this the semiotic consideration that the concept of jing is suspended in dense cultural âwebs of significanceâ,153 one is left with the essential âuntranslatabilityâ of jing.154
Meaning in CM tends to be inherently flexible. Hsu has pointed out that classical CM education teaches âdifferent meanings in particular contextsâ and points out âthe basic rule for reading classical Chinese textsâthat what was valid in one context was not in anotherâ.155 Unlike biomedicine, such polysemy is not viewed as problematic in CM: âThe senior doctor Zhang made no attempt whatsoever to try to reconcile these different meaningsâ.156 The Western translators of CM seem to continue such a tradition. Lyttleton, for instance, initially glosses jing as gametes, but without any overt acknowledgement or signposting jing comes to represent âthe potential for gamete developmentâ (rather than the gamete itself), âthe function of the ovaries and some aspects of pituitary functionâ, and one of âthe ânutrientsâ required for an egg to developâ.157 The term thus moves from form to function and object to process, demonstrating significant semantic fluidity.
For some, such flexibility captures the overlapping holistic nature of reality and exposes the falsehood in the tendency of science to present reality in terms of immutable objects and fixed meanings. For others, however, it exposes CM as an example of what Karl Popper defined as pseudo-science.158 In this view, the principles of CM, like Marxism or Freudian psychoanalytic theory, can be made to explain any clinical data whatsoever and are thus unfalsifiableâand therefore unscientific. Such semantic fluidity in the hands of CM authors is frequently extrapolated cross-paradigm, allowing them to be inappropriately (from the scientific perspective) creative with biomedical âfactsâ (see below).
The concept of jing thus eludes straightforward definition in English, and its scope goes beyond a label for any particular physical structureâas Bromley et al., point out, âJing is both adjective and noun, vital and vitality, essence and essentialâ.159 Hsu creatively bridges such linguistic shortcomings by coining the composite term âsubstance-forceâ to describe jing.160 The concept of jing thus includes aspects of form/substance and function/process. Just like the seed of a plant, jing is at once a spatial object as well as being the potential of other future forms. Whilst not âaliveâ in the same way as the grown plant, a seed remains dormant, awaiting activation by the right conditions. Similarly, jing is rooted in the physical, but its primary raison dâetre is of future generation and enfoldment.
Jing and clinical practice
What are clinicians to do with such confusion? One might follow the example of Professor Li Yueqing, a modern CM andrologist, who so fully embraces the clinical relevance of semen analysis that for him âneither the patientâs self-sensation . . . nor his tongue show us any reliable signs . . . the microscopic examinations are the only way to make differentiationâ.161 Or one may agree with Farquhar and resist such modern distortion of CM theory: âChinese medical thinking is not naturally murky, it just gets that way when one attempts to fill its intellectual objects (patterns of pathological function) with anatomical contentâ.162 Professor Liâs bold statement points to a very modern problemâthat ever since Chinese doctors were able to look through a lens at sperm (or indeed at eggs or ovaries), it became clear that not all patients with infertility show explicit signs of the âKidney deficiency with insufficient essenceâ that for Professor Li constitute the âfundamental causative factor of male infertilityâ.163 However they think about them, modern CM practitioners working in reproductive medicine face a barrage of biomedical test results proffered by increasingly well-informed patients who expect their practitioner not only to understand them, but also to intervene successfully in order to influence them. Such tests have become the standard method to assess the effects of CM treatment modern reproductive research.164 As a practitioner, one might welcome the advantages provided by such clinical information, and respond by improvising an âintegratedâ diagnosis and treatment.165 Indeed, one perspective on what has happened to CM since the arrival of biomedicine in China is that, rather than distortion, such integrative improvisation represents innovation.166 Now that CM finds itself in the post-genomic era, practitioners of CM are frequently required to respond to new discoveries. Horne, for example, presents innovative theories regarding epigenetics, even suggestingâcontentiouslyâthat a womanâs body may even be able to produce fresh eggs.167
There are, however, dangers associated with attaching CM so closely to biomedicine, as recently persuasively documented by Scheid in the case of menopause.168 To downgrade empirical clinical knowledge built over centuries in favour of the tangible presence of âjingâ as seen through a microscope risks losing potentially effectiveâalbeit at times theoretically precariousâclinical strategies that had developed prior to the paradigm shift. For instance, the shift in womenâs reproductive medicine from focusing primarily on the blood (as jing) to focusing more on the eggs (as jing) entails changing the primary clinical strategy from nourishing blood to nourishing jing. Such theoretical complications are not unique in CM; in some ways this mirrors the long-running debate in Chinese medicine about the respective roles of the Heart and brain in terms of housing the shen (spirit), where new theories simply began to coexist withârather than replaceâthe old theories.169 Such âgraftingâ of the new on to the old is typical of the development of CM.170
Double standards
The discourse of modern practitioners of CM is apparently very different to their biomedical peers, who at times brutally pronounce171 on a womanâs reproductive capacity based on clinical tests, despite these tests having a modest-to-poor predictive capacity.172 Lewis states that biomedicine âcan do little to helpâ in cases of premature ovarian failure, whilst for the CM practitioner the condition is ârewardingâ, backing up this assertion with the polemic force of a patient diagnosed as âirreversibly infertileâ by her Western medicine doctor who was helped to conceive with CM.173 Lewis markets her services to a client group that biomedical consultants would view as irremediably infertile and beyond even the help of ART, so that women âwhose FSH values are well over 100 . . . [and] . . . whose AMH values were zero conceive naturallyâ.174 To such patients a diagnosis of jing deficiency is potentially less terrifying than âovarian failureâ for both patient and practitioner, especially given the existence of herbs and acupuncture points thatâtheoretically at leastâincrease jing. Lewis rejects the biomedical view of the reproductive system as an âever-deteriorating disease process waiting for interventionâ and instead views it through the âdifferent lensâ of Chinese medicine, in which the body-mind-spirit is imbued with âmiraculousâ abilities and the overall context is given as, âThereâs no such thing as infertilityâ.175 Despite reframing pathology through a âdifferent lensâ, however, Lewisâ descriptions of the reproductive system remain cast in biomedical terms: âFSH is the flame. The uterus is the oven. LH is the opening of the flue. The ovaries are the wood.â176 This displays the tendency of practitioners of CM to cherry-pick from biomedical theory when it suits their purposesâthus the title of Lewisâ book, The Infertility Cure,177 is couched in biomedical terms, and her discourse about infertility is replete with biomedical explanations of the pathomechanisms involved, thus conferring biomedical authority on her work. Despite her frequent rejections of biomedical discourse, however, her CM is informed by the same questionable biomedical scripts identified in recent scholarship by Scheid:178 âmenopausal symptoms can be alleviated when the Kidney system is tonified or stimulated, thus augmenting the Essence.â179
Conclusions
This paper demonstrates that the term jing is used in a variety of ways across modern English-language sources according to the specific context and particular agenda of the author. This supports Hsuâs contention that âDifferent contexts of social practice have been shown to modify the connotation, pragmatic use, and performative significance of Chinese medical termsâ.180 Not only is the term polysemous in itself, it is associated with a tangle of overlapping terms that are used interchangeably and inconsistently. In light of these issues, this paper puts forward the following conclusions and recommendations:
Clinicians should be aware that glossing jing as the human gametes, whilst clinically pragmatic, narrows the concept to become congruent with modern biomedical scripts. In particular, such a reading loses the functional/processual aspects of the term, as well as the vital âverticalâ relationship of jing with shen that is potentially significant in terms of treatment. This paper therefore concurs with Farquhar, that âTo give both Chinese and Western medicine their due requires finer discriminations of the specific relations between objects and processes, products and relations of production, spatial and temporal materialities.â181
Although the comparison of CM with biomedicine should be approached cautiously, due to unequal underlying power relations, the correspondence of jing with gametes, DNA, and stem cells is alluring.182 Investigating the effects of traditional CM jing-strengthening strategies on such possible biomedical correlates of jing constitutes a potentially fertile field of research. In terms of reproductive medicine this may involve investigating the effects of acupuncture and CHM strategies to augment jing and strengthen the Kidneys for conditions of low egg reserve, premature ovarian failure, azoospermia, and high DNA fragmentation, amongst others. Given the lack of biomedical options available for poor egg/embryo quality and high sperm DNA fragmentation rates,183 CM strategies to tonify jing may be able to assist childless couples affected by such conditions, and therefore warrants further research.
The conceptual boundaries between jing and other technical terms within CMâsuch as the Kidneyâare indistinct. Scholarship to investigate how such distinctions operate, particularly within pre-Han and Han primary medical texts, would be valuable in this regard.
Authors of CM texts should be vigilant of the limitations of the English language and the western dualistic mindset when dealing with the concept of jing, and take responsibility for clarifying their particular reading of the term. It is recommended that the term be left in its original Chinese to allow for semiotic freedom.
This paper concludes by reiterating the metaphor conveyed to Farquhar by her Chinese teacher, in which classic texts of CM are likened to the bamboo that is flexible enough to be made into both a toothpick and a house.184 The concept of jing shares such conceptual flexibility, and clinicians, scholars, and researchers should remain mindful of this.
* An abridged version of this article was published in The Journal of Chinese Medicine, Issue 98 (February 2012). The author would like to thank Professor Volker Scheid, whose sage guidance made the writing of this paper possible, enjoyable, and illuminating.
1 For example, see Maciocia 2005.
3 Hammer 1999.
4 Zhang and Rose 1999.
6 For example, see Maciocia 2005.
10 Lyttleton 2004.
12 Crimmel et al. 2001; Deadman 2008.
14 Jones and Lopez 2006.
15 Daniluk 2001; Peterson et al. 2007.
18 Strauss and Corbin 1990.
19 Aronson 1994.
20 Ezzy 2002.
21 Braun and Clarke 2006.
22 Strauss and Corbin 1990.
24 Kukla 1999.
25 Wiseman and Zhang 2003.
29 Hammer 1999.
30 Lin and Flaws 1991.
31 Zhang and Rose 1999.
32 Furth and Châen 1992.
34 Ross 1984.
35 Larre and Rochat de la Vallée 1999.
38 Lyttleton 2004.
39 Lyttleton 2004, p. 373.
40 Heese 2006.
41 Unschuld 2005, p. 52.
42 Yang and Liu 1995, p. 52.
43 Jin 1999, p. 186.
44 For example, see Geng et al. 2010.
45 Furth and Châen 1992.
46 Noll and Wilms 2009, p. 108.
47 Furth 1999.
48 Farquhar 1991.
49 Furth and Châen 1992.
50 Lyttleton 2004, p. 262.
51 Liang 2003.
52 Magidoff 2000.
53 Damone 2008.
55 Horne 2011.
56 Wiseman and Feng 1998.
57 Liang 2003, p. 7.
58 Betts 2006.
59 Lyttleton 2004.
60 Furth 1999.
62 Farquhar 1987.
64 Cheng 1987.
66 Larre and Rochat de la Vallée 1999.
67 Damone 2008, p. 68.
68 Larre and Rochat de la Vallée 1999.
69 Horne 2011.
71 Liu and Liu 2009.
72 Porkert 1974.
73 Noll and Wilms 2009, p. 311.
76 Flaws 1989.
77 Lyttleton 2004, p. 338.
78 Lyttleton 2004, p. 13.
79 Lyttleton 2004.
82 See Noll and Wilms 2009.
83 Damone 2008.
84 Liu 2005, p. 23.
85 Neal-Perry and Santoro 2006.
86 Lyttleton 2004.
88 Wu 2010, p. 96.
89 Liang 2003, p. 79.
90 Lewis 2011a.
91 Horne 2011.
93 Jin 1999.
94 Lyttleton 2004, p. 119.
96 Lewis 2004, p. 174.
97 Lewis 2004, p. 178.
98 Farquhar 1991.
99 Lewis 2004.
101 Horne 2011.
102 Xingzhe 2004a.
103 Elliott 2009.
104 West 2011.
105 Heese 2006.
106 Liang 2003.
107 Liu and Liu 2009.
108 Hammer 1999.
109 Lin and Flaws 1991.
110 Flaws 1989.
113 Lyttleton 2004, p. 339.
114 Wu 2010.
116 Lyttleton 2004, p. 262.
117 Wu 2010, p. 94.
119 Unschuld 2003, p. 53.
121 Xingzhe 2004a.
122 Furth 1987.
123 Furth 1999.
124 Larre and Rochat de la Vallée 1999.
125 Lyttleton 2004.
126 Larre and Rochat de la Vallée 1999.
127 Damone 2008.
130 Lewis 2011b.
131 Noll and Wilms 2009.
133 Scheid 2002a.
134 Farquhar 1987.
136 Karchmer 2004.
138 Liang 2003.
139 Li 2005.
141 Magner 2005.
142 Andrews 1996.
143 Farquhar 1987.
145 Zhang and Rose 1999.
146 Farquhar 1987.
147 Larre and Rochat de la Vallée 1999.
148 Farquhar 1987.
149 Wu 2010.
153 Geertz 1973.
154 Kovacs 1989.
155 Hsu 1999.
157 Lyttleton 2004.
158 Okasha 2002.
160 Hsu 1999.
161 Li 2005.
162 Farquhar 1991.
163 Li 2005.
164 For example, see Geng et al. 2010.
166 Karchmer 2004.
167 Horne 2011.
170 Andrews 1996.
173 Lewis 2004, p. 239.
174 Lewis 2011b.
175 Lewis 2011a.
177 Lewis 2004.
179 Lewis 2004, p. 30.
180 Hsu 1999.
181 Farquhar 1991.
182 Karchmer 2004.
183 Carrell and Peterson 2010.
184 Farquhar 1987.
References
AAOM Asian Medical Nomenclature Debates 2006 Sacramento AAOM
Andrews B. J. âThe Making of Modern Chinese Medicine, 1895â1937â 1996 Cambridge Gonville and Caius College PhD Dissertation
Aronson J. âA Pragmatic View of Thematic Analysisâ The Qualitative Report 1994 [Accessed 21 May 2011] 2 1 available from: <http://www.nova.edu/ssss/QR/BackIssues/QR2-1/aronson.html>
Atwood W. & Dobkin S. âStorm Clouds are Coming: Ways to Help Couples Reconstruct the Crisis of Infertilityâ Contemporary Family Therapy 1992 14 5 385 403
Baker G. & Morris K. J. Descartesâ Dualism 1996 London Routledge
Bensky D. , Gamble A. & Clavey S. et al. Materia medica: Chinese Herbal Medicine 2004 3rd edition Seattle Eastland Press
Bensky D. , Blalack J. & Chase C. et al. âToward a Working Methodology for Translating Chinese Medicineâ The Lantern 2006 3 3 10 16
Betts D. The Essential Guide to Acupuncture in Pregnancy & Childbirth 2006 Hove Journal of Chinese Medicine Press
Boyatzis R. E. Transforming Qualitative Information: Thematic Analysis and Code Development 1998 Thousand Oaks, CA Sage Publications
Braun V. & Clarke V. âUsing Thematic Analysis in Psychologyâ Qualitative Research in Psychology 2006 3 77 101
Broekmans F. J. , Kwee J. & Hendriks D. J. et al. âA Systematic Review of Tests Predicting Ovarian Reserve and IVF Outcomeâ Human Reproduction Update 2006 12 6 685 718
Bromley M. , Freeman D. & Hext A. et al. Jing shen: A translation of Huainanzi chapter 7 2010 London Monkey Press
Brown L. Yangsheng: Nourish Life 2009 [Accessed 21 May 2011] Available from: <http://www.acubalance.ca/fertility-diet/acubalance-fertility-diet/yangsheng-nourish-life>
Brown L. Repeated Unsuccessful IVF Cycles and Diminished Ovarian Reserveâhow Chinese Medicine Provides Hope 2011 [Accessed 14 June 2011] Available from: <http://acubalance.ca/repeated-unsucessful-ivf-cycles-and-diminished-ovarian-reserve-how-chinese-medicine-provides-hope>
Buck C. , Rose K. & Felt R. âOn Terminology and Translationâ Journal of Chinese Medicine 2000 63 38 52
Carrell D. T. & Peterson M. Reproductive Endocrinology and Infertility: Integrating Modern Clinical and Laboratory Practice 2010 New York Springer
Chao S. L. , Huang L. W. & Yen H. R. âPregnancy in Premature Ovarian Failure after Therapy using Chinese Herbal Medicineâ Chang Gung Medical Journal 2003 26 6 449 452
Cheng X. N. Chinese Acupuncture and Moxibustion 1987 Beijing Foreign Languages Press
Clavey S. âNotes on the Treatment of Male Infertilityâ Journal of Chinese Medicine 2003 73 45 52
Crimmel A. S. , Conner C. S. & Monga M. âWithered yang: A Review of Traditional Chinese Medicine Treatment of Male Infertility and Erectile Dysfunctionâ Journal of Andrology 2001 22 2 173 182
Damone B. Principles of Chinese Medical Andrology 2008 Boulder Blue Poppy Press
Daniluk J. C. The Infertility Survival Guide 2001 Oakland, CA New Harbinger Publications
Deadman P. âThe Treatment of Male Subfertility with Acupuncture Journal of Chinese Medicine 2008 88 5 16
Deadman P. , Al-Khafaji M. & Baker K. A Manual of Acupuncture 1998 Hove Journal of Chinese Medicine Publications
Dharmananda S. Kidney Water no date [Accessed 13 June 2011] Available from: http://www.itmonline.org/5organs/kidney.htm
Elliott D. âThe Treatment of Elevated FSH Levels with Chinese Medicineâ Journal of Chinese Medicine 2009 91 5 11
Ernst E. âComplementary Medicine: Common Misconceptionsâ Journal of the Royal Society of Medicine 1995 88 5 244 247
Ezzy D. âQualitative Analysis: Practice and Innovationâ 2002 Crows Nest, Australia Allen & Unwin
Farquhar J. âProblems of Knowledge in Contemporary Chinese Medical Discourseâ Social Science and Medicine 1987 24 1013 1021
Farquhar J. âObjects, Processes, and Female Infertility in Chinese Medicineâ Medical Anthropology Quarterly 1991 5 4 370 399
Flaws B. Endometriosis, Infertility and Traditional Chinese Medicine 1989 Boulder Blue Poppy Press
Flaws B. Fulfilling the Essence: A Handbook of Traditional Contemporary Chinese Treatments for Female Infertility 1993 Boulder Blue Poppy Press
Furth C. âConcepts of Pregnancy, Childbirth, and Infancy in Chiâing Dynasty Chinaâ The Journal of Asian Studies 1987 46 1 7 35
Furth C. âA Flourishing Yin: Gender in Chinaâs Medical Historyâ 1999 Berkeley, CA University of California Press 960 1665
Furth C. & Châen S. âChinese Medicine and the Anthropology of Menstruation in Contemporary Taiwanâ Medical Anthropology Quarterly 1992 6 1 27 48
Geertz C. âThick Description: Toward an Interpretive Theory of Cultureâ The Interpretation of Cultures: Selected Essays 1973 New York Basic Books
Geng S. S. , Li H. Z. & Wu X. K. et al. âEffect of wujijing Oral Liquid on Menstrual Disturbance of Womenâ Journal of Ethnopharmacology 2010 128 3 649 653
Greening D. âFrequent Ejaculation. A Pilot Study of Changes in Sperm DNA Damage and Semen Parameters using Daily Ejaculationâ Fertility and Sterility 2007 88 1 19 20
Guo B. & Powell A. Listen to your Body: The Wisdom of the dao 2001 Hawaii University of Hawaii Press
Hammer L. âThe Paradox of the Unity and Duality of the Kidneys according to Chinese Medicine: Kidney Essence, yin, yang, qi, the mingmenâTheir Origins, Relationships, Functions and Manifestationsâ American Journal of Acupuncture 1999 [Accessed 13 June 2011] 27 3&4 available from; <http://www.dragonrises.edu/wp-content/themes/dragon/downloads/articles/hammer-kidneyduality.pdf>
Heese I. âThe Egg Factor: Using Chinese Herbal Medicine to Improve Egg Quality in a 45-year-old Womanâ Journal of Chinese Medicine 2006 82 36 41
HFEA Fertility Facts and Figures 2008 London Human Fertilisation and Embryology Authority
Horne B. Optimising Ovarian Reserve 2011 [Accessed 13 June 2011] Available from: <http://prodseminars.adobeconnect.com/p21685638/?launcher=false&fcsContent=true&pbMode=normal>
Hsu E. The Transmission of Chinese Medicine 1999 Cambridge Cambridge University Press
Jensen T. K. , Jørgensen N. & Asklund C. âFertility Treatment and Reproductive Health of Male Offspring: A Study of 1,925 Young Men from the General Populationâ American Journal of Epidemiology 2007 165 583 590
Jin W. X. Diagnosis of Sterility and its Traditional Chinese Medicine Treatment 1999 Jinan Shandong Science and Technology Press
Jones R. E. & Lopez K. H. Human Reproductive Biology 2006 3rd edition Amsterdam Academic Press
Kai C. M. , Main K. M. & Andersen A. N. et al. âReduced Serum Testosterone Levels in Infant Boys Conceived by Intracytoplasmic Sperm Injectionâ Journal of Clinical Endocrinology and Metabolism 2007 92 2598 2603
Kaptchuk T. Chinese Medicine: The Web that has no Weaver 2000 London Rider
Karchmer E. I. Orientalizing the Body: Postcolonial Transformations in Chinese Medicine 2004 Ann Arbor, MI UMI
Ke S. K. âTreating Infertility in Traditional Chinese Medicineâ European Journal of Oriental Medicine 2008 6 1 10 11
Kovacs J. Unschuld P. âLinguistic Reflections of the Translation of Chinese Medical Textsâ Approaches to Chinese Medical Literature 1989 Boston Kluwer Academic Publishers 85 96 1989
Kukla A. Social Constructivism and the Philosophy of Science 1999 London Routledge
Larre C. & Rochat de la Vallée E. Essence Spirit Blood and Qi 1999 London Monkey Press
Larre C. & Rochat de la Vallée E. âJing Essenceâ European Journal of Oriental Medicine 2002 [Accessed 13 June 2011] 4 1 Available from: http://www.ejom.co.uk/vol-4-no-1/featured-article/jing-essence.html
Leung H. Y. , Chiu P. Y. & Poon M. K. T. et al. âA yang-invigorating Chinese Herbal Formula Enhances Mitochondrial Functional Ability and Antioxidant Capacity in Various Tissues of Male and Female Ratsâ Rejuvenation Research 2005 8 4 238 247
Lewis R. The Infertility Cure 2004 London Little, Brown and Company
Lewis R. High FSH 2011a [Accessed 13 June 2011] Available from: <http://thefertilesoul.com/chinese_medicine/>
Lewis R. AMHâwhat does it really mean? (part 1) 2011b [Accessed 13 June 2011] Available from: <http://thefertilesoul.com/chinese_medicine/>
Li H. S. âProf. Li Yueqingâs Experience in Treating Male Infertilityâ Journal of Traditional Chinese Medicine 2005 25 2 122 124
Liang L. F. Acupuncture & IVF: Increase IVF Success by 40â60% 2003 Boulder Blue Poppy Press
Lin A. & Flaws B. The Dao of Increasing Longevity and Conserving Oneâs Life: A Handbook of Traditional Chinese Geriatrics and Chinese Herbal Patent Medicines 1991 Boulder Blue Poppy Press
Liu F. W. Shuai X. Z. & Flaws B. The Essence of Liu Feng-wuâs Gynecology 1998 Boulder Blue Poppy Press
Liu G. H. Warm Pathogen Diseases: A Clinical Guide 2005 Seattle Eastland Press
Liu Z. & Liu L. Essentials of Chinese Medicine 2009 London Springer
Lyttleton J. Treatment of Infertility with Chinese Medicine 2004 Edinburgh Churchill Livingstone
Maciocia G. Obstetrics & Gynecology in Chinese Medicine 1999 Edinburgh Churchill Livingstone
Maciocia G. The Foundations of Chinese Medicine. A Comprehensive Text for Acupuncturists and Herbalists 2005 2nd edition Edinburgh Churchill Livingstone
Magidoff A. âIn Search of a Philosophical Medicineâ California Journal of Oriental Medicine 2000 11 2 29 33
Magner L. N. A History of the Life Sciences 2005 3rd edition New York Marcel Dekker, Inc.
Marchment R. Gynaecology Revisited 2007 Sydney Churchill Livingstone
Neal-Perry G. & Santoro N. F. Neill J. D. âAging in the Hypothalamic-pituitary-ovarian Axisâ Knobil & Neillâs Physiology of Reproduction 2006 St Louis Elsevier 2729 2758
Noll A. A. & Wilms S. Chinese Medicine in Fertility Disorders 2009 Stuttgart Thieme
Okasha S. Philosophy of Science. A very short introduction 2002 Oxford Oxford University Press
Peterson B. D. , Newton C. R. & Feingold T. âAnxiety and Sexual Stress in Men and Women Undergoing Infertility Treatmentâ Fertility & Sterility 2007 88 4 911 914
Porkert M. The Theoretical Foundations of Chinese Medicine 1974 Cambridge, MA MIT Press
Qian H. M. , Fan X. Y. & Chen Y. Y. âDr Chen Ying-yiâs Experience in Treating Premature Ovarian Failureâ Journal of Traditional Chinese Medicine 2010 30 3 217 221
Qian Z. Y. âMale Infertility: Three Cases Treated by Acupunctureâ Journal of Chinese Medicine 1997 53 26 27
Ross J. Zang Fu. The Organ Systems of Chinese Medicine 1984 Edinburgh Churchill Livingstone
Scheid V. âRemodeling the Arsenal of Chinese Medicine: Shared Pasts, Alternative Futuresâ Annals of the American Sociological Association: Global Perspectives on Complementary and Alternative Medicine 2002a 583 136 159
Scheid V. Chinese Medicine in Contemporary China: Plurality and Synthesis 2002b Durham Duke University Press
Scheid V. âTraditional Chinese MedicineâWhat are we Investigating? The Case of Menopauseâ Complementary Therapies in Medicine 2007 15 1 54 68
Scheid V. âGlobalising Chinese Medical Understandings of Menopauseâ East Asia Science, Technology and Society: An International Journal 2009 2 4 485 496
Scheid V. , Bensky D. & Ellis E. et al. Formulas & Strategies 2009 2nd edition Seattle Eastland Press
Sivin N. Traditional Medicine in Contemporary China 1987 Michigan University of Michigan Centre for Chinese Studies
Strauss A. & Corbin J. Basics of Qualitative Research: Grounded Theory Procedures and Techniques 1990 Newbury Park, CA Sage Publications, Inc.
Tempest H. G. , Homa S. T. & Zhai X. P. et al. âSignificant Reduction of Sperm Disomy in Six Men: Effect of Traditional Chinese Medicine?â Asian Journal of Andrology 2005 7 4 419 425
Tortora G. J. & Derrickson B. H. Principles of Anatomy and Physiology 2005 11th edition Chichester John Wiley & Sons
Unschuld P. U. Medicine in China: A History of Ideas 1985 Berkeley University of California Press
Unschuld P. U. Nan ching: The Classic of Difficult Issues 1986 Berkeley University of California Press
Unschuld P. U. Huang di nei jing su wen: Nature, Knowledge, Imagery in an Ancient Chinese Medical Text 2003 Berkeley University of California Press
Unschuld P. U. Chinese Life Sciences. Traditional Readings in Classical Chinese Medicine 2005 Berkeley University of California Press
West Z. AMH, DHEA, help!! 2011 [Accessed 13 June 2011] Available from: <http://www.zitawest.com/blog/category/low-ovarian-reserve/>
Wing T. A. & Seidlmeier E. S. âMeasuring the Effectiveness of Chinese Herbal Medicine in Improving Female Infertilityâ Journal of Chinese Medicine 2006 80 22 28
Wiseman N. & Feng Y. A Practical Dictionary of Chinese Medicine 1998 Brookline Paradigm Publications
Wiseman N. & Zhang Y. H. Chinese Medical Characters Basic Vocabulary 2003 vol. 1 Brookline Paradigm Publications
World Health Organisation WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region 2007 Manila World Health Organisation
Wu Y. L. Reproducing Women: Medicine, Metaphor, and Childbirth in Late Imperial China 2010 Berkeley University of California Press
Xingzhe X. Y. âNourishing Lifeâ The Lantern 2004 [Accessed 13 June 2011] 1 1 Available from: <http://www.thelantern.com.au/resource_detail.php?id=19>
Xingzhe X. Y. âYangsheng: The Thing about jingâ The Lantern 2004a [Accessed 13 June 2011] 1 2 Available from: http://www.thelantern.com.au/resource_detail.php?id=55
Xutian S. , Zhang J. & Wozniak L. âNew Exploration and Understanding of Traditional Chinese Medicineâ American Journal of Chinese Medicine 2009 37 3 411 426
Yang S. Z & Liu D. W. Fu Qing-zhuâs Gynecology 1995 Boulder Blue Poppy Press
Zelicha K. & Nuria U. âPoor Ovarian Reserve and High FSH Levelsâ The Lantern 2010 7 2 6 10
Zhang H. H. & Rose K. Who Can Ride The Dragon? An Exploration of the Cultural Roots of Traditional Chinese Medicine 1999 Brookline Paradigm Publications
Zhang L. âDr Shi Hanzhangâs Experience in Treating Andropathyâ Journal of Traditional Chinese Medicine 2007 27 4 284 287
Zhang T. L. & Flaws B. Zhejiang College of Traditional Chinese Medicine A Handbook of Traditional Chinese Gynecology 1995 Boulder Blue Poppy Press
Zollman C. & Vickers A. âComplementary Medicine and the Patientâ British Medical Journal 1999 319 1486
Appendices
Appendix 1: Detailed search strategy
Appendix 2: Extended quotations and definitions of jing
Huang Di Nei Jing Su Wen, Chapter 1
âWhen a girl is fourteen, she comes into her prenatal vitalities [tiangui], her controller vessel moves and her thoroughfare vessel is abundant; her menses flow regularly and she is able to bear children. . . . When [a boy] is sixteen, his kidney qi is abundant and he comes into his prenatal vitalities. His seminal essence overflows and drains; he is able to unite yin and yang and so beget youngâ. (translated by Wu 2010, p. 90)
Nan Jing (Difficult Issue 36)
â(1) Each of the depots is a single [entity], except for the kidneys which represent a twin [entity]. Why is that so?
(2) It is like this. The two kidneys are not both kidneys. The one on the left is the kidney; the one on the right is the gate of life. (3) The gate of life is the place where the spirit-essence lodges; it is the place to which the original influences are tied. (4) Hence, in males it stores the essence; in females it holds the womb. (5) Hence one knows there is only one kidney.â (translated by Unschuld 1986)
World Health Organisation 2007
1.2.1 essence ç²¾ (1) the fundamental substance that builds up the physical structure and maintains body function; (2) reproductive essence stored in the kidney
1.2.2 innate essence å 天ä¹ç²¾ the original substance responsible for construction of the body and generation of offspring, often referring to the reproductive essence, also called prenatal essence
1.2.3 acquired essence å¾å¤©ä¹ç²¾ the essential substance acquired from the food after digestion and absorption, and used to maintain the vital activities and metabolism of the body, the same as postnatal essence
1.2.4 kidney essence è ç²¾ the original essence stored in the kidney
Wiseman and Feng 1998
âEssence ç²¾ jing: That which is responsible for growth, development, and reproduction, and determines the strength of the constitution, and is manifest physically in the male in the form of semen. Essence is composed of earlier heaven essence (congenital essence) which is inherited from the parents and constantly supplemented by later heaven essence (acquired essence) produced from food by the stomach and spleen.â
Maciocia 2005
âJing is said to be stored by the Kidneys (with which it has a close relationship), and controls birth, growth, reproduction and general constitutional strength.â
Sivin 1987
âThe Ching is the foundation of life; it is a fundamental substance that shapes the human body and maintains every kind of vital activity, directly affecting growth, development, aging, and death.â
Shanghai College of Traditional Medicine 1981
âEssence (a Yin characteristic) is that aspect of the body which is the basis for all growth, development and sexuality. Congenital Essence is that part of the bodyâs Essence which is inherited from the parents. After birth this Essence, which is akin to an inborn constitution, determines each of our growth patterns. Congenital Essence can never be replaced if lost, but can be supplemented by acquired Essence, which is derived from food. Essence also has the narrow meaning of semen.â
Dharmananda n.d.
âJing is the Chinese designation for the essential fluid of our physical body. . . . The basic yin (matter) from which all yang (physical action) springs is jing. In classical Chinese medical texts, jing is sometimes referred to as the bodyâs âoriginal waterâ with water representing the ultimate yin (âoriginal fireâ being the ultimate yang). . . . Although the word jing is synonymous with the Chinese word semen, the seminal fluid represents only one form of jing. Other dense fluid essences such as saliva (particularly the kind that gets spontaneously excreted during meditation), vaginal fluids, breast milk or blood are all regarded to be different transformations of one and the same jing; these are refined essences.â
Kaptchuk 2000
âThe texture most closely associated with life itself; it is the source of life and its unfolding. . . . It is the texture that gives organic life its specific character. It is the stuff of growth and development. Essence is the potential for differentiation into lifeâs Yin and Yang. Essence, in one form or another, is the primordial seed of the life process, the life process itself, and lifeâs final fruit.â
- 1
For example, see Maciocia 2005.
- 2
Andrews 1996; Scheid 2002a; Karchmer 2004.
- 3
Hammer 1999.
- 4
Zhang and Rose 1999.
- 5
See Flaws 1989 and Ross 1984.
- 6
For example, see Maciocia 2005.
- 7
Lyttleton 2004; Jin 1999.
- 10
Lyttleton 2004.
- 11
Heese 2006; Horne 2011.
- 13
Lewis 2004; Horne 2011.
- 14
Jones and Lopez 2006.
- 16
Lewis 2011a; Horne 2011.
- 17
Zollman and Vickers 1999; Ernst 1995.
- 18
Strauss and Corbin 1990.
- 19
Aronson 1994.
- 20
Ezzy 2002.
- 21
Braun and Clarke 2006.
- 22
Strauss and Corbin 1990.
- 24
Kukla 1999.
- 25
Wiseman and Zhang 2003.
- 26
Liang 2003; Maciocia 2005.
- 28
See Unschuld 1986; Wu 2010; Hammer 1999.
- 29
Hammer 1999.
- 30
Lin and Flaws 1991.
- 31
Zhang and Rose 1999.
- 32
Furth and Châen 1992.
- 34
Ross 1984.
- 35
Larre and Rochat de la Vallée 1999.
- 37
World Health Organisation 2007.
- 38
Lyttleton 2004.
- 39
Lyttleton 2004, p. 373.
- 40
Heese 2006.
- 41
Unschuld 2005, p. 52.
- 42
Yang and Liu 1995, p. 52.
- 43
Jin 1999, p. 186.
- 45
Furth and Châen 1992.
- 46
Noll and Wilms 2009, p. 108.
- 47
Furth 1999.
- 48
Farquhar 1991.
- 49
Furth and Châen 1992.
- 50
Lyttleton 2004, p. 262.
- 51
Liang 2003.
- 52
Magidoff 2000.
- 53
Damone 2008.
- 55
Horne 2011.
- 56
Wiseman and Feng 1998.
- 57
Liang 2003, p. 7.
- 58
Betts 2006.
- 59
Lyttleton 2004.
- 60
Furth 1999.
- 61
Tortorra and Derrickson 2005, p. 1094.
- 62
Farquhar 1987.
- 64
Cheng 1987.
- 66
Larre and Rochat de la Vallée 1999.
- 67
Damone 2008, p. 68.
- 68
Larre and Rochat de la Vallée 1999.
- 69
Horne 2011.
- 71
Liu and Liu 2009.
- 72
Porkert 1974.
- 73
Noll and Wilms 2009, p. 311.
- 74
Horne 2011; West 2011; Lewis 2004.
- 76
Flaws 1989.
- 77
Lyttleton 2004, p. 338.
- 78
Lyttleton 2004, p. 13.
- 79
Lyttleton 2004.
- 80
Tortorra and Derrickson 2005, p. 1073.
- 81
Tortorra and Derrickson 2005, p. 1094.
- 82
See Noll and Wilms 2009.
- 83
Damone 2008.
- 84
Liu 2005, p. 23.
- 85
Neal-Perry and Santoro 2006.
- 86
Lyttleton 2004.
- 88
Wu 2010, p. 96.
- 89
Liang 2003, p. 79.
- 90
Lewis 2011a.
- 91
Horne 2011.
- 93
Jin 1999.
- 94
Lyttleton 2004, p. 119.
- 95
Heese 2006; Ke 2008; Brown 2009.
- 96
Lewis 2004, p. 174.
- 97
Lewis 2004, p. 178.
- 98
Farquhar 1991.
- 99
Lewis 2004.
- 101
Horne 2011.
- 102
Xingzhe 2004a.
- 103
Elliott 2009.
- 104
West 2011.
- 105
Heese 2006.
- 106
Liang 2003.
- 107
Liu and Liu 2009.
- 108
Hammer 1999.
- 109
Lin and Flaws 1991.
- 110
Flaws 1989.
- 111
Kaptchuk 2000; Hammer 1999; Scheid 2007.
- 112
Noll and Wilms 2009, p. 29; Guo and Powell 2001, p. 139.
- 113
Lyttleton 2004, p. 339.
- 114
Wu 2010.
- 116
Lyttleton 2004, p. 262.
- 117
Wu 2010, p. 94.
- 118
Greening 2007; Damone 2008.
- 119
Unschuld 2003, p. 53.
- 121
Xingzhe 2004a.
- 122
Furth 1987.
- 123
Furth 1999.
- 124
Larre and Rochat de la Vallée 1999.
- 125
Lyttleton 2004.
- 126
Larre and Rochat de la Vallée 1999.
- 127
Damone 2008.
- 129
Horne 2011; Lewis 2004.
- 130
Lewis 2011b.
- 131
Noll and Wilms 2009.
- 133
Scheid 2002a.
- 134
Farquhar 1987.
- 135
Andrews 1996; Karchmer 2004.
- 136
Karchmer 2004.
- 137
Andrews 1996; Karchmer 2004.
- 138
Liang 2003.
- 139
Li 2005.
- 141
Magner 2005.
- 142
Andrews 1996.
- 143
Farquhar 1987.
- 145
Zhang and Rose 1999.
- 146
Farquhar 1987.
- 147
Larre and Rochat de la Vallée 1999.
- 148
Farquhar 1987.
- 149
Wu 2010.
- 150
AAOM 2006.
- 153
Geertz 1973.
- 154
Kovacs 1989.
- 155
Hsu 1999.
- 157
Lyttleton 2004.
- 158
Okasha 2002.
- 160
Hsu 1999.
- 161
Li 2005.
- 162
Farquhar 1991.
- 163
Li 2005.
- 166
Karchmer 2004.
- 167
Horne 2011.
- 168
Scheid 2007; Scheid 2009.
- 170
Andrews 1996.
- 171
Lewis 2004; Atwood and Dobkin 1992.
- 173
Lewis 2004, p. 239.
- 174
Lewis 2011b.
- 175
Lewis 2011a.
- 177
Lewis 2004.
- 178
Scheid 2007; Scheid 2009.
- 179
Lewis 2004, p. 30.
- 180
Hsu 1999.
- 181
Farquhar 1991.
- 182
Karchmer 2004.
- 183
Carrell and Peterson 2010.
- 184
Farquhar 1987.

{kind=link}