Abstract
Many healthy people complain of functional gastrointestinal (GI) tract symptoms that do not fit diagnostic criteria for established diseases. Disrupted intestinal microbiomes are associated with these functional conditions, thus the use of beneficial bacteria shown to restore the protective microbiome may be useful. Our aims were to determine if Heyndrickxia (Bacillus) coagulans GBI-30, 6086 (BC30) would improve GI functions in healthy adults living in China and to determine its effect on the GI microbiome. Healthy adults (
1 Introduction
Functional gastrointestinal (FGIDs) disorders are commonly found in healthy adults: 16% of generally healthy people complain of functional dyspepsia and 17-20% complain of lower gastrointestinal (GI) disorders, such as constipation or loose stools (Ford, 2020; Kaminski et al., 2020). FGID currently lacks a standardised definition and is diagnosed mainly based on symptoms, which may encompass a wide diversity of intestinal complaints including functional idiopathic constipation, altered bowel function or increased frequency of stools, irritable bowel syndrome (IBS), dyspepsia or intestinal gas (Ford et al., 2014a; Kaminski et al., 2020; Rathi et al., 2024). Many diverse factors such as diet, lifestyle behaviours, medications, travel, health status, stress or living conditions may impact normal GI functions and often are associated with disrupted normal microbiome profiles (Black et al., 2020; Kaminski et al., 2020; Shin et al., 2019). While many treatments are available for prolonged GI conditions, such as irritable bowel syndrome (IBS) or inflammatory bowel disease (IBD), there are no standard treatments for FGIDs, but therapies that involve the restoration of the normal GI microbiome are currently being explored, including increasing dietary fibre and the use of probiotics or foods supplemented with beneficial bacteria (Kaminski et al., 2020; Rathi et al., 2024; Shin et al., 2019).
Probiotics are living microbes that confer a health benefit on the host, particularly in relation to gastrointestinal function where their efficacy is supported by a growing body of evidence most commonly (Kumar et al., 2020a; Sniffen et al., 2018). Specific strains have been found effective for the treatment of different GI disorders including IBS, antibiotic associated diarrhoea or travelerâs diarrhoea (Ceccherini et al., 2022; Fan et al., 2022; Ford et al., 2014; Guglielmetti et al., 2011; McFarland et al., 2021; Sniffen et al., 2018; Tian et al., 2017; Wen et al., 2020). However, it should be noted that the efficacy of probiotics is both disease-specific and strain-specific, thus efficacy must be based on studies focused on identical strain(s) or having appropriate sub-group analyses (McFarland et al., 2018). As probiotics are widely available in foods or beverages, or as dietary supplements or over-the-counter products, their use has shifted from treating patients to broader applications in generally healthy people as an aid to improve GI health and functioning (Bodke et al., 2022; Merenstein et al., 2024).
The evidence based on randomised controlled clinical trials for specific strains of probiotics for FGIDs is limited. Three meta-analyses have been conducted for functional constipation but only a few probiotic strains had significant evidence of improved symptoms, and the conclusions were based on a small number of trials (Ford et al., 2014; Kaminski et al., 2020; Zhang et al., 2020). A review of current guidelines for idiopathic constipation concluded there are insufficient numbers of trials with the same strain or strains to make a valid conclusion of efficacy and more trials were recommended (Bassotti et al., 2021).
At least ten different Bacillus coagulans strains have been screened for their potential role in FGID and mechanism of action studies showed promise (Adibpour et al., 2019; Altun et al., 2021; Cao et al., 2020). Based on randomised, controlled trials B. coagulans Unique IS-2 was effective for IBS (Madempudi et al., 2020), acute pediatric diarrhoea (Dutta et al., 2011) and functional abdominal pain (Saneian et al., 2015). Two other strains showed improvement in IBS symptoms: B. coagulans LBSC (Rathi et al., 2024) and B. coagulans MTCC (Majeed et al., 2023). B. coagulans GBI-30, 6089 improved intestinal gas in one trial (Kalman et al., 2009), improved dyspepsia in another trial (Kuman et al., 2020b) and three trials found improved symptoms in IBS (Abhardi et al., 2020; Dolin et al., 2009; Hun et al., 2009).
Several taxonomic reclassifications of this species have occurred over the years. The genus and species were originally known as Lactobacillus sporogenes, then revised to Bacillus coagulans Dutta et al., 2011). In 2020 it was reclassified as Weizmannia coagulans (including strain GBI-30, 6086) (Fijan et al., 2023), and in 2023 it was finally reclassified as Heyndrickxia coagulans GBI-30, 6086 (Narsing et al., 2023). Following the recommendation to gather more data on specific strains that may improve GI tract functions, we focused on one strain, H. coagulans GBI-30, 6086 (BC30), a lactic-acid producing, spore-forming, Gram-positive facultative anaerobic bacterium first isolated in 1915 from spoiled canned milk and identified as Lactobacillus sporogenes (Cao et al., 2020). Pharmacokinetic studies found BC30 spores survived gastric acid and bile acids with 51% of the oral dose reaching the intestine (Keller et al., 2019). This strain does not permanently colonize the intestine and was cleared 4-5 days after discontinuation (Salvetti et al., 2016). BC30 spores are highly resistant to heat with an optimum growth temperature of 35-50 °C and survive well in various foodstuffs (ranging from cheese, orange juice, chocolate, yogurt and bread) (Soares et al., 2019). BC30 has several mechanisms of action that improve intestinal function: (1) production of enzymes facilitating protein digestion and aiding stool excretion (Jager et al., 2018; Stecker et al., 2020), (2) increasing the absorption of amino acids (Stecker et al., 2020; Walden et al., 2024), (3) improving the beneficial intestinal microbiome (Cao et al., 2020; Nyangale et al., 2014; Nyangale et al., 2015), (4) regulating the immune system (Anaya-Loyola et al., 2019; Fitzpatrick et al., 2011; Gepner et al., 2017; Yang et al., 2014), and (5) supporting GI and digestive health (Dolin, 2009; Hun, 2009; Kalman et al., 2009).
The safety of this strain has been well documented in acute and chronic toxicity studies and was found to be well tolerated in humans in doses as high as 9Â Ã 1012/day and no transfers of antibiotic-resistant genes have been found (Endres et al., 2009; Salvetti et al., 2016). Only two randomised trials with BC30 for functional intestinal symptoms have been done in Caucasians and both reported significant improvements in intestinal symptoms (Kalman et al., 2009; Kumar et al., 2020b). Our trial is the first to be studied in a Chinese population with FGID.
The aims of this study are to evaluate the efficacy of Heyndrickxia (Bacillus) coagulans GBI-30, 6086 (BC30) to improve GI tract functioning in otherwise healthy adults and to evaluate the impact of BC30 on the intestinal microbiome.
2 Materials and methods
Recruitment of participants
Non-hospitalised healthy adults were recruited from July 2021 to October 2021 using notices posted at Beijing hospital and notices sent out to the public. Participants were screened and study visits were conducted at one site (Beijing Hospital, China).
Study design
The study used a prospective parallel group design, with a 2-week screening/run-in period and then participants were randomised (1:1) to either BC30 or placebo for four weeks. No follow-up was done after the study intervention was discontinued. The study protocol was carried out according to standardised methods, as recommended in the SFDA Green Book (Ministry of Health, 2003) and retrospectively registered with clinicaltrials.gov (NCT06644001) on October 16, 2024 and the protocol is available here. The study protocol was approved by the ethics committee at Beijing Hospital and informed consent was obtained from all participants. The study protocol and reporting were done following the CONSORT guidelines (CONSORT checklist, Supplementary Table S1) (Moher et al., 2010). The data collected included standard PICOS data: (1) population (age), (2) intervention (powder rehydrated in beverage at daily dose of 1 sachet/day, for 28 days), (3) comparisons (placebo, blinded), (4) primary outcomes: intestinal function (symptoms, stool frequency and consistency) and changes in intestinal microbiome and (5) secondary outcomes (safety data, quality of life).
Inclusion criteria included: adults (18-65 years old), generally healthy but with irregular bowel movements, including <4 stools/week or periodic (over 2/week) loose stools. Participants were asked to refrain from consuming any other probiotic or bacterial dietary supplements during the 2-week run-in period and during the 4-week study period. Exclusion criteria included: aged <18 or >65 years, pregnant or lactating women, susceptible to allergens or having food allergies, existing diseases (cardiovascular, cerebrovascular, hepatic, renal, hematopoietic, endocrine), mentally ill patients, constipation symptoms induced by surgical operation within the past 30 days, acute intestinal tract diseases in the past 30 days, constipation symptoms induced by severe organ lesion (colon cancer, severe enteritis, intestinal obstruction, IBD, etc.), inability to ingest oral study treatments, administered relevant products recently which would affect the outcome of the study (probiotic or prebiotic substances in the past month), diagnosed with organic GI diseases in the past month or taken antibiotics in the past month. Exclusion criteria during the study period included: not compliant with study protocols, discontinuation of the study treatment, or ingestion of supplements or medicines during the trial which would affect the outcome of the study (including dietary supplements, fibre, prebiotics, antibiotics, laxatives, etc.) and participants providing incomplete data.
The randomisation scheme was done using a random number table and no blocked design was used. Both BC30 and control interventions were produced by Bioflag Biotech (Anhui, China) in identical appearing packages. Study personnel (including study intervention allocator, medical study staff, outcome assessors, analysis team) and participants were blinded as to which intervention they received.
A 2-week run-in period was done to train participants to fill out the daily diary forms and to discontinue any ingestion of other probiotics or excluded medications from their diet. Four visits with study personnel were conducted during the study (from Day â14 to Day 29). The screening visit (Day â14) was conducted to evaluate eligibility, collect informed consent and medical history data. Eligible participants were asked to complete Health Daily Diaries, which recorded their daily stool count and consistency and any adverse reactions (Supplementary Form S1). Data on quality of life, GI tract symptoms and routine health assessment data (blood pressure and heart rate) were collected during the run-in period (Days â14 to â1). No study treatments were given during the screening/run-in period. At the second visit (baseline, Day 0), participants filled out questionnaires on intestinal symptoms and quality-of-life. Eligible participants received their blinded study treatments at this visit. Participants were instructed to begin taking one sachet daily, at approximately the same time of day, and to continue for the duration of the study. Participants were provided with sufficient product at visits to cover the time between visits. Routine health assessment data (blood pressure and heart rate) were collected. Blood and urine samples were collected to assess safety. A faecal sample was collected for microbiome enumeration. At the first follow-up visit (Day 14), daily diaries were reviewed for GI symptoms, compliance to study protocol was assessed (sachet counts and any history of exclusionary medications) and questionnaires on intestinal symptoms and quality of life were completed. Blood pressure and heart rate were measured. A faecal sample was collected for microbiome evaluation. At the end-of-study visit (Day 29), daily dairies were collected and any residual study treatments returned. Questionnaires on intestinal symptoms and quality of life were completed. Blood pressure and heart rate were measured. A faecal sample was collected for microbiome evaluation. Blood and urine samples were collected to assess safety parameters.
Study intervention
Heyndrickxia (Bacillus) coagulans GBI-30, 6086 (BC30) (Kerry Ingredients Trading, Shanghai, China) was given as a sachet with maltodextrin (1.93Â g) and BC30 (0.07Â g) powder (1Â Ã 109 spores/day) rehydrated in a beverage. The BC30 powder was dissolved in cold water and administered orally. The placebo sachet consisted of maltodextrin (2Â g) and the powder was dissolved in cold water and administered orally. Both the appearance and taste of BC30 and the placebo were identical. Both study treatments are stable at room temperature. Study treatments were given for four weeks.
Primary outcomes
As FGID lacks a standardised definition, we defined FGID for our trial based on recommended diagnostic criteria including adults with irregular bowel movements, which may include constipation (<4 stools/week) or occasional diarrhoea or loose stools (>2 loose stools/week) or dyspepsia. Primary outcomes included improvements in GI functions (change of stool frequency or consistency or changes in intestinal symptom scores) and changes in the intestinal microbiome.
Primary outcomes relating to intestinal functions. Five different outcome measures for GI functions were analysed (measurement of stool frequency, presence of constipation, fecal consistency, defection effort and GI symptom scores). Data was collected from the Health Daily Diary for stool frequency, constipation, faecal consistency and defection effort (Supplementary Form S1), or from the Gastrointestinal Symptom Rates Scale (GSRS) for GI symptoms scores (Supplementary Form S2), or from Severity Of Dyspepsia Assessment (SODA) for upper GI symptoms (Supplementary Form S3) during the 2-week run-in period and during the study (Weeks 1-4). Stool frequency was defined as the number of stools per day. Constipation was defined as present if <4 stools/week and absent if ±4 stools/week were noted. Fecal consistency was measured using a modified Bristol Stool Scale (BSS), which defines three types of stool consistencies (Yang et al., 2008). Fecal characteristics were scored as 0 = smooth sausage shaped with or without cracks, 1 = sausage-shaped with lumps and 2 = separated, hard lumps. Daily measurements were averaged by participant for each study week. Defection effort (symptoms during defection) data was scored as: 0 = normal stool habit, 1 = defection with mild discomfort, 2 = defection with discomfort and difficulty, or 3 = defection with frequent abdominal pain or burning. Daily measurements were averaged by participant for each study week. The severity of GI symptoms was measured using the GSRS, which contains 15 items, each rated on a four-point Likert scale ranging from no discomfort to severe discomfort (Revicki et al., 1997). Based on a factor analysis, the 15 GSRS items break down into the following five domains: abdominal pain (abdominal pain, hunger pains and nausea); reflux (heartburn and acid regurgitation), diarrhoea (diarrhoea, loose stools and urgent need for defecation), indigestion (borborygmus, abdominal distension, eructation and increased flatus) and constipation (constipation, hard stools and feeling of incomplete evacuation). The scores were calculated by taking the mean of the items completed within an individual scale, with higher scores indicating greater severity of symptoms (Kulich et al., 2008; Revicki et al., 1997). The overall GSRS score was computed as the average of all five sub-scores. Upper GI tract symptoms were measured using the SODA, which is scored on four items (dyspepsia, heartburn, reflex, nausea) depending upon the frequency of the symptoms (1 = none/week, 2 = 1 time/week, 3 = 1-2 times/week, 4 = 3-4 times/week and 5 = once a day or more) (Rabeneck, 2003).
Primary outcomes related to the changes in intestinal microbiota
Total genome DNA from samples was extracted using CTAB/SDS method. DNA concentration and purity was monitored on 1% agarose gels. PCR amplification of the V3-V4 region of 16S rRNA gene was performed using universal primers 341F (5â²-CCTAYGGGRBGCASCAG-3â²) and 806R (5â²-GGACTACNNGGGTATCTAAT-3â². Sequencing libraries were generated using TruSeq® DNA PCR-Free Sample Prepara-tion Kit (Illumina, USA) following manufacturerâs recommendations. The library quality was assessed on the Qubit@2.0 Fluorometer (Thermo Scientific) and Agilent Bioanalyzer 2100 system. The library was then sequenced on an Illumina NovaSeq platform and 250 bp paired-end reads were generated.
Paired-end reads were assigned to samples based on their unique barcode, truncated by cutting off the barcode and primer sequence and then, combined using FLASH software (VI.2.7) (Magoc et al., 2011). Quality filtering on the raw tags was performed to obtain the high-quality clean tags using QIIME (V1.9.1) (Caporas et al., 2010). Tags were compared with the reference database (Silva database v138) using UCHIME algorithm to detect chimera sequences that were removed (Edgar et al., 2011). Effective tags obtained were then clustered with 97% identity and resulting operational taxonomic units (OTUs) were annotated using the Silva v138 and the Mothur method (Chappidi et al., 2019). Relative abundances were reported, which is the percent composition of an organism to the total number of organisms de-tected. If a species of interest, such as lactobacillus, is too low (<103), the values presented in the tables may be reported as relative abundances multiplied by 103.
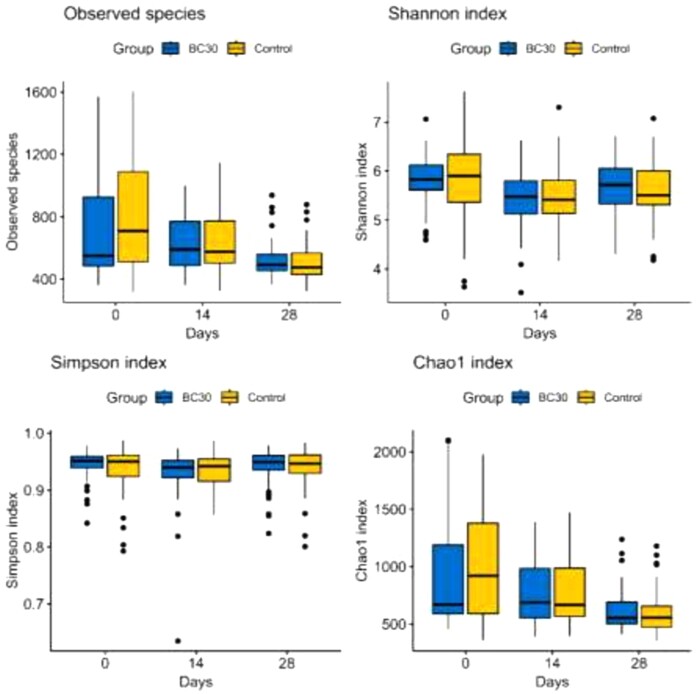
Alpha Diversity indexes (Chao1, Simpson and Shannon) were computed using Quiime (v1.9.1) to analyse the diversity of microbial communities within a sample. Chao1 estimates the total number of species contained in the microbiota sample and the higher the Chao1 index indicates more species are present at low concentrations in the microbiota. Simpson index represents the diversity and evenness of species distribution in the microbiota and a higher Simpson index indicates a high degree of evenness. The Shannon index indicates the total number and proportion of taxa present, with the higher the Shannon index indicating a higher diversity and more uniform the species distribution.
Secondary outcomes
Quality of life (QoL) was assessed during the SF-36.v2 questionnaire at three visits (Day 0, Day 14, Day 29). The SF-36 version 2 consists of 11 items covering eight domains of health (physical functioning, limitations due to physical health, pain, general health, energy, social functioning, limitations due to emotional problems and emotional well-being). Items were scored according to the frequency of symptoms or degree of impact on daily functioning, as shown in Supplementary Form S4 (Ware, 2000).
Safety
Routine blood, urine and fecal tests were conducted before (Day 0) and after (Day 29) study interventions. Chest X-ray, abdominal b-ultrasound, ECG, liver (aspartate aminotransferase (AST), alanine aminotransferase (ALT) and bilirubin) and kidney function (urea, creatinine) assays, lipid profiles and blood glucose levels were also done at these two visits. In addition, participants were asked to fill out diaries noting any adverse reactions during the study using their Health Daily Diaries. Vital signs (blood pressure, heart rate) were collected at all study visits.
Statistical analysis
Sample size was determined according to the requirement in the Ministry of Healthâs Green Book (Ministry of Health, 2003), which states a minimum of 50 participants per group is required for clinical trials. No interim analysis was planned. Data was grouped by intervention group (BC30 or placebo). SPSS software and R statistical computing version 4.3.2 (R Foundation for Statistical Computing) were used for statistical analysis. The P-value was set to â¤0.05 as significant (two-tailed) for all analyses. No imputation was used for missing data. Categorical outcomes were presented as an absolute number and percentage and analysed with the Chi2 test or Fisherâs exact test if cell size was <5. Continuous outcomes were presented as mean ± standard deviations. Intragroup changes (within each study group BC30 or control) were analysed using the Cochranâs Q test for categorical variables and the Friedman test for quantitative variables. Intergroup changes (changes between the two study groups) were assessed at each time point using ANOVA or the Wilcoxon Mann-Whitney test (Zou et al., 2023). The âabsolute changeâ measured the change in outcome measures from baseline visit to study end (visit at Week 4) between the two groups and was analysed with the Wilcoxon Mann-Whitney test. To compare the longitudinal trends in changes of GI symptoms between the two study groups over time (Baseline to Week 4), linear mixed models (LMMs) with random intercepts and slopes were used, including age and sex as covariates and an interaction term (group â time). For microbiome analyses, LMM models were used with sequencing batch included as an additional covariate. Difference of âTrends over timeâ (slopes) were presented as an adjusted beta coefficients with 95% confidence intervals (OR, 95% CI) from the interaction term, indicating the difference between groups in the average weekly change of the dependent quantitative variable. For the presence of constipation, a logistic mixed model was set and adjusted odds ratio and 95% CI (OR, 95% CI) for the interaction term was reported, reflecting the relative change in the odds of being constipated between treatment arms.
3 Results
Recruitment
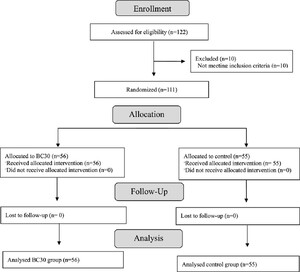
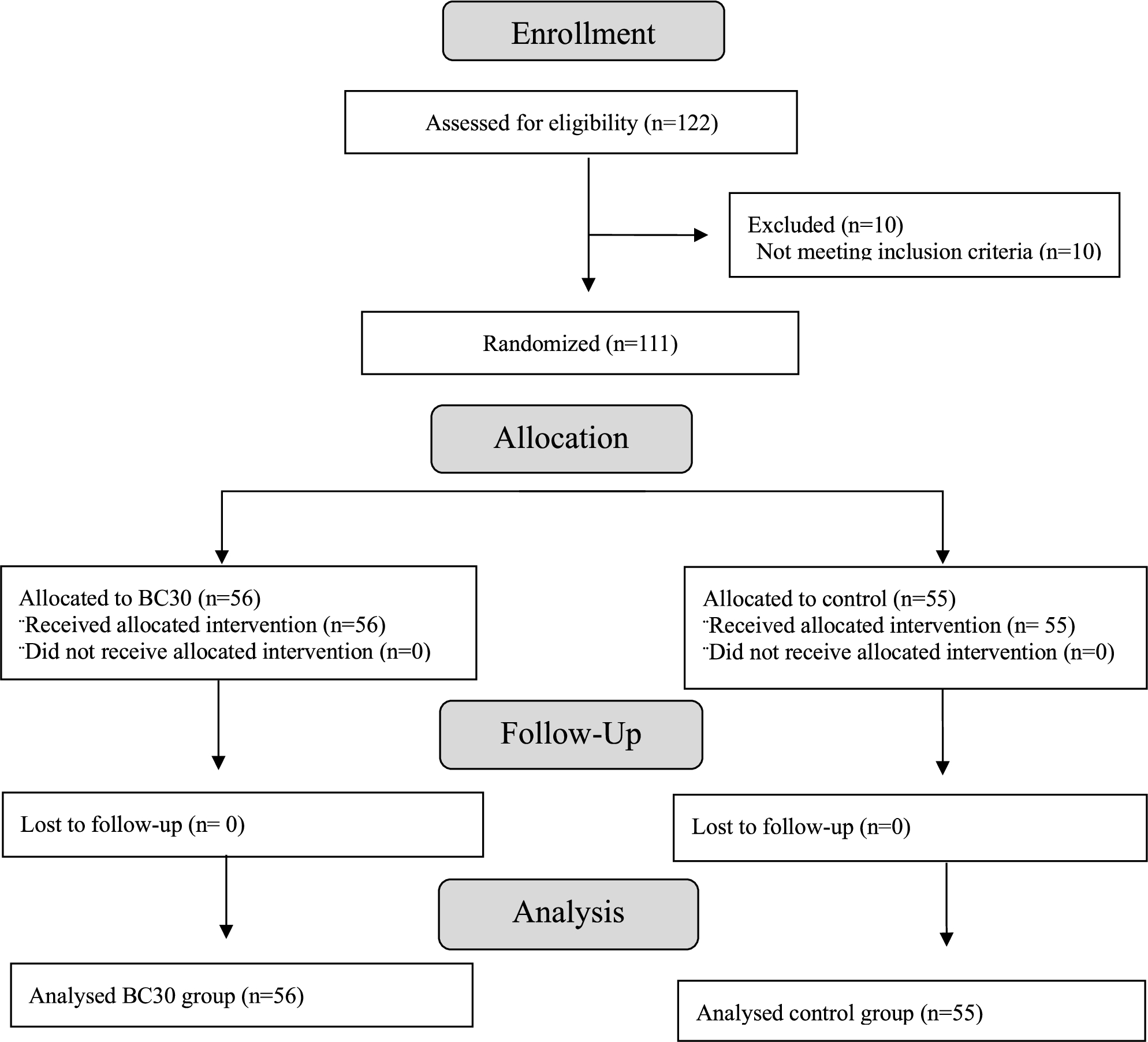
A total of 122 healthy adults were screened and 111 were enrolled, while 10 were not eligible (Figure 1). There was 0% attrition during the trial. No interim analysis was carried out nor were there any deviations to the study protocols or procedures during the study.

CONSORT study flowchart.
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
Baseline characteristics
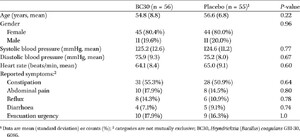
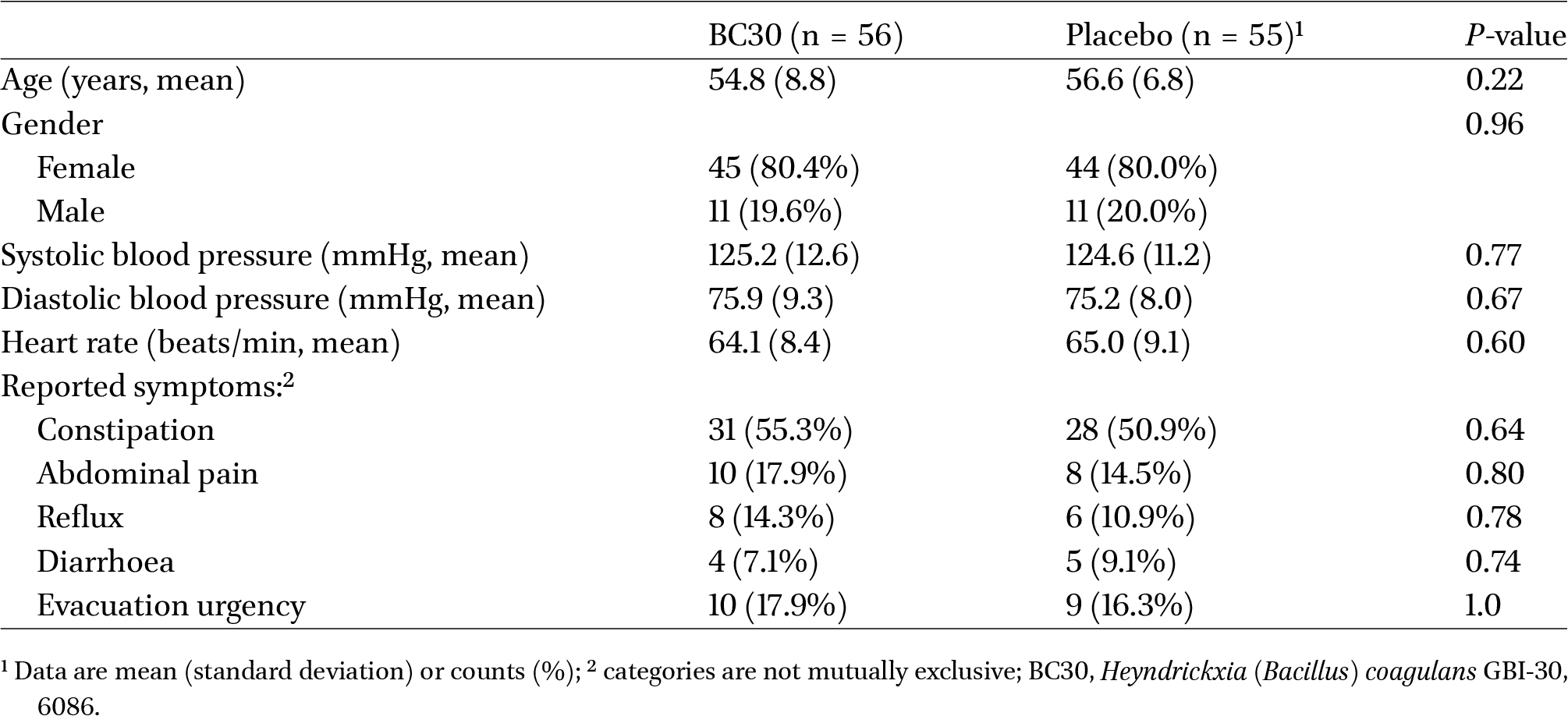
There were no significant differences in demographic characteristics (age, gender), vital signs (blood pressure, heart rate) or reported GI symptoms between the two study groups (Table 1).
Comparison of demographic and clinical characteristics of the two study groups at baseline (Day 0)1
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
Effect on GI functions
Intestinal function and symptoms were analysed by several indicators for the BC30 group (
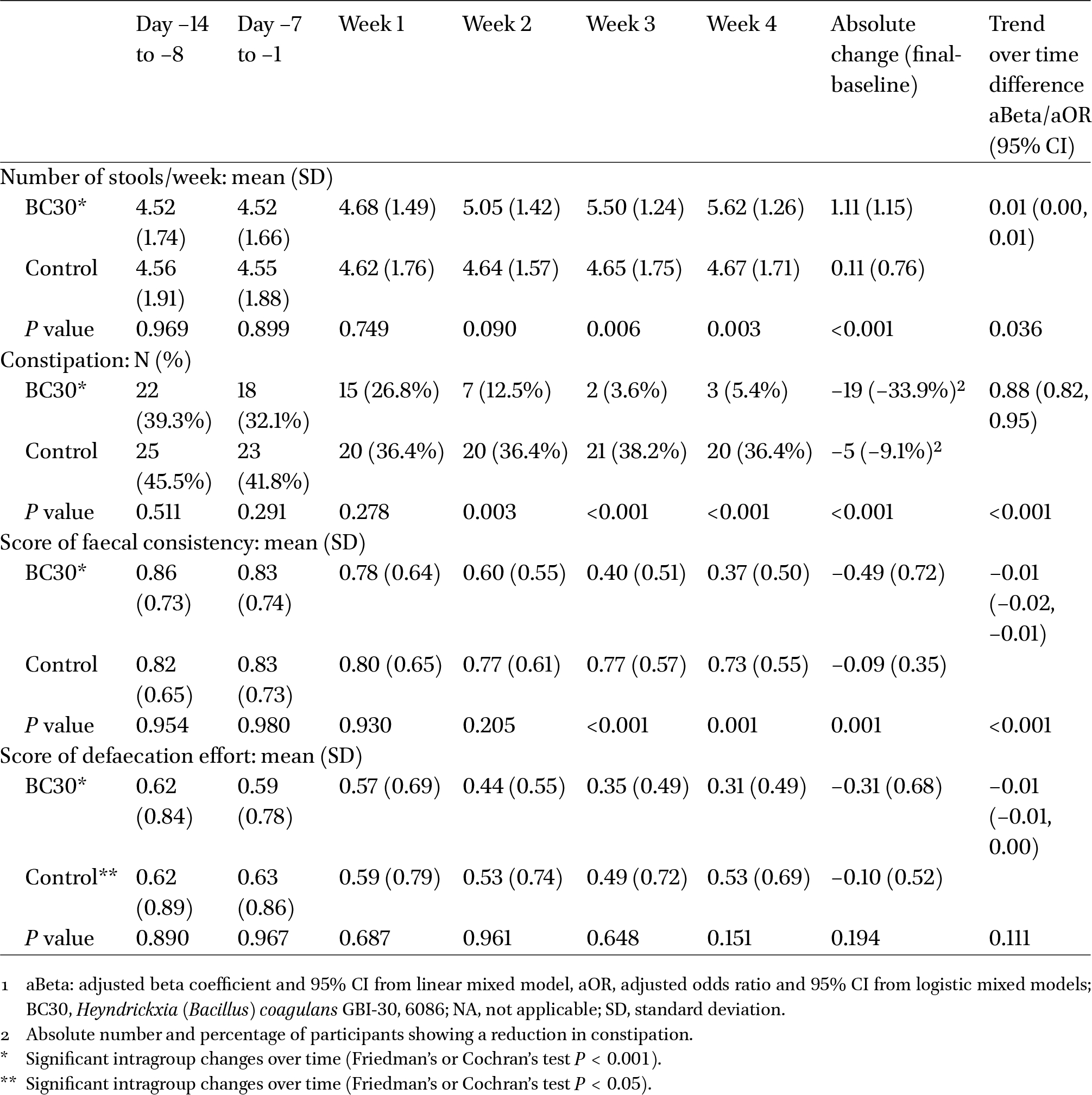
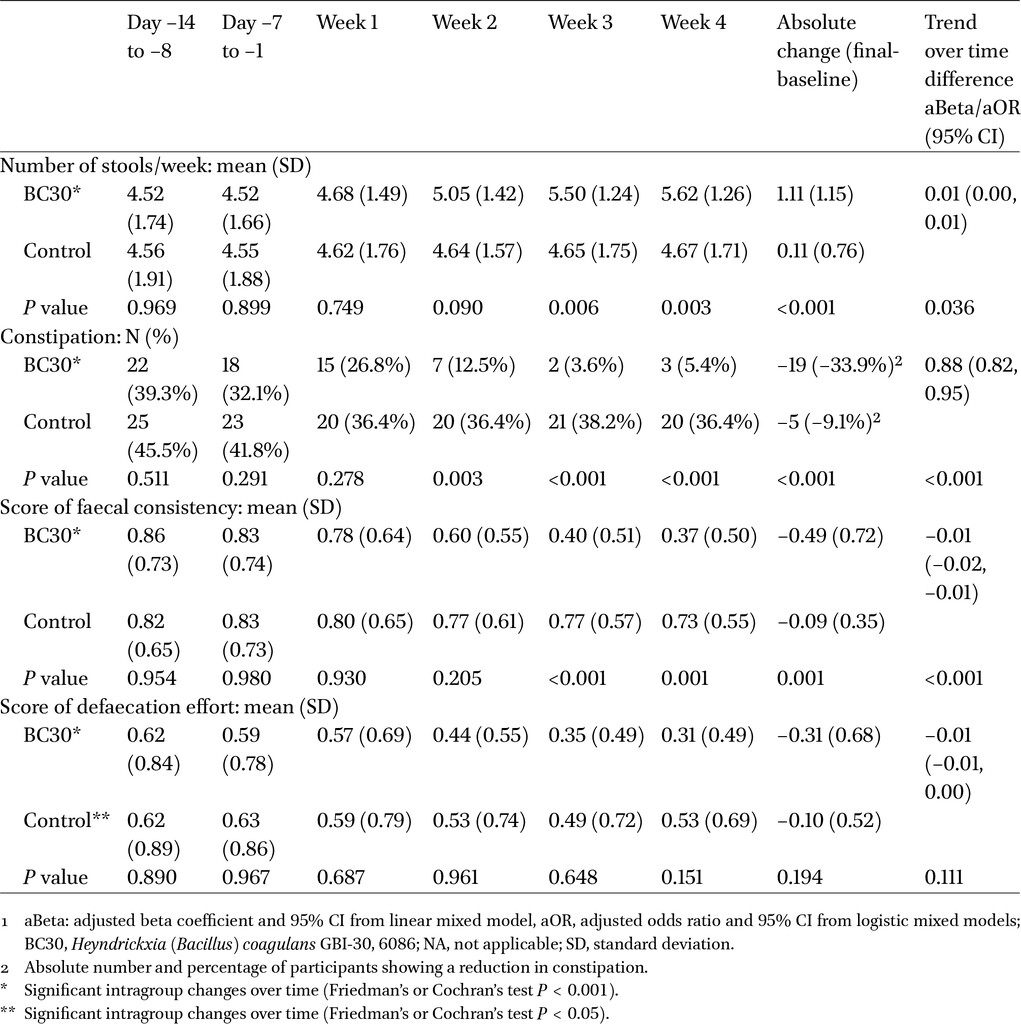
Comparison of intestinal function indicators between the BC30 group (
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
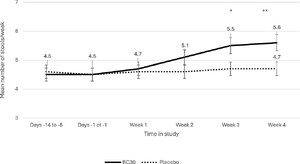
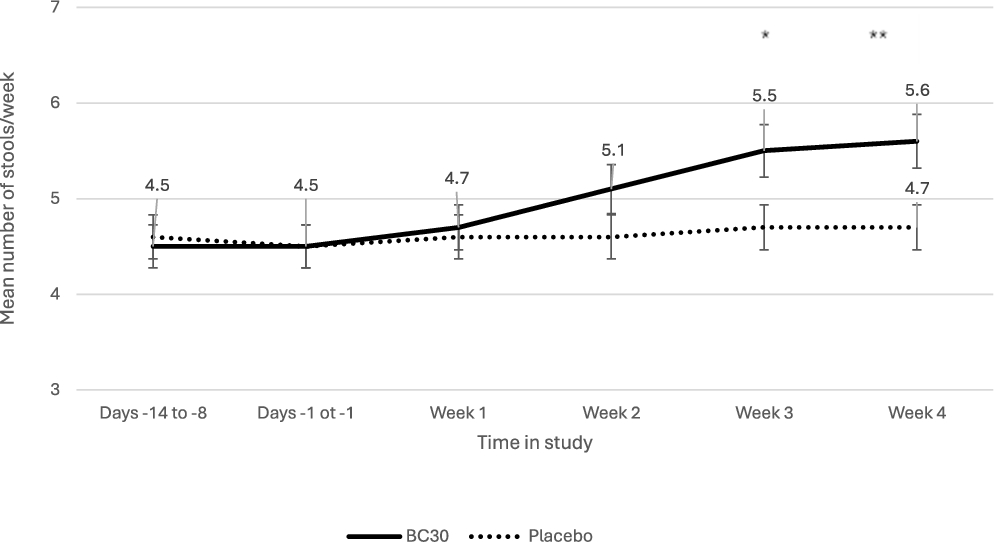
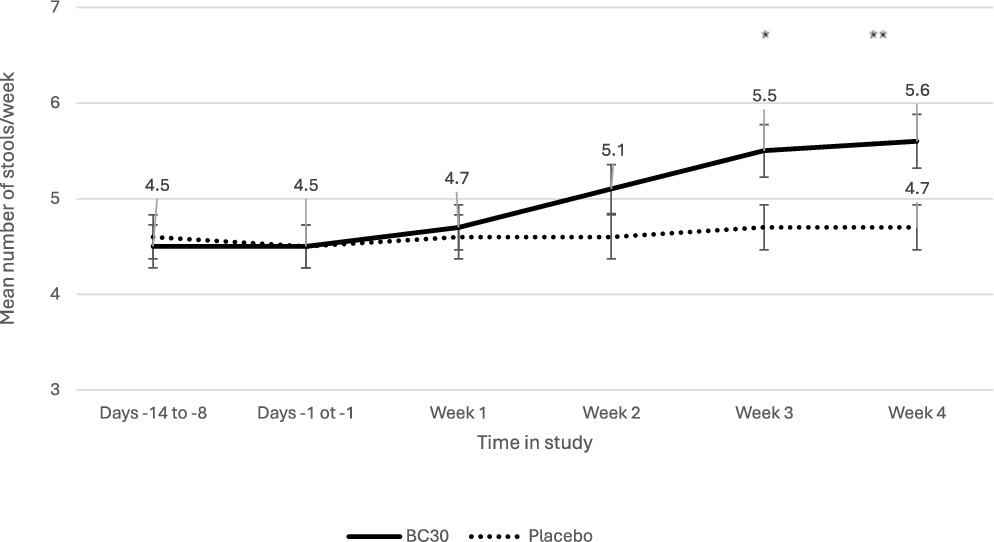
Stool frequency/week linearly increased in the BC30 group compared with the control group during the study (
The frequency of constipation also decreased over time (
Faecal consistency scores significantly improved during the study (
There was no significant difference found in the scores of defection effort for the BC30 group compared to the control group (Table 2).
Comparison of mean number of stools/week by study period between BC30 group and placebo control group. *
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
There was also a significant improvement in overall GSRS score in the BC30 group compared with the control group, but only during the last two weeks of the study, as shown in Table 3. The absolute change of the overall GSRS score from baseline to the end of the study was significantly reduced for BC30 (â0.19 ± 0.29,
Comparison of intestinal function indicators between the BC30 group (
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
BC30 had no significant effect on upper GI tract symptoms as measured by the SODA questionnaire. The mean scores for dyspepsia, heartburn, reflux and nausea were not significantly different for the two study groups at any time-period (Supplementary Table S2).
Impact on GI microbiome
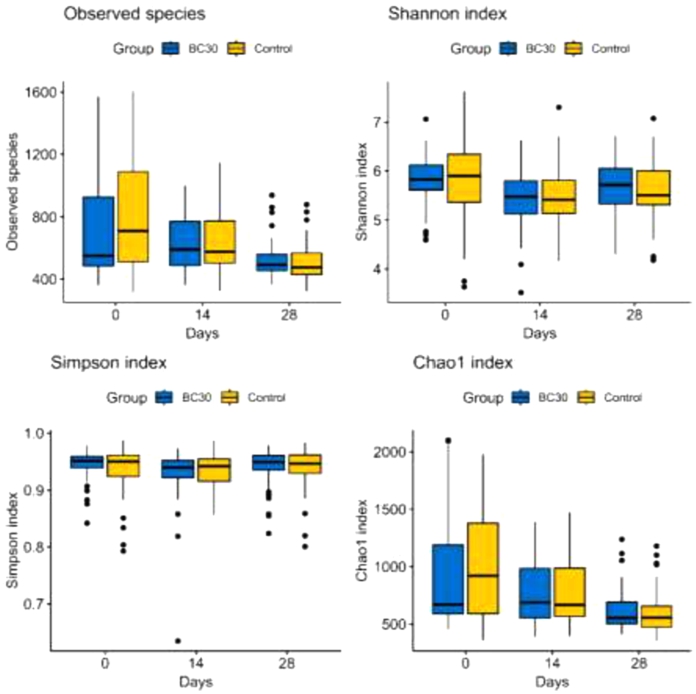
During the study, diversity was assessed and a similar reduction in the number of species was found in the faecal microbiome as measured by the Shannon diversity index and Chao1 diversity index in both study groups (Figure 3, Supplementary Table S3).
While the final number of observed species and the Shannon index were slightly less for the BC30 group at the end of the intervention, no significant differences between groups were observed overall or at each time point.
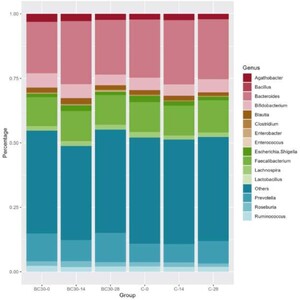
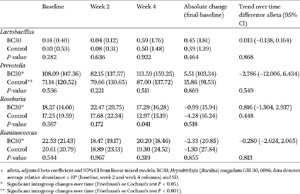
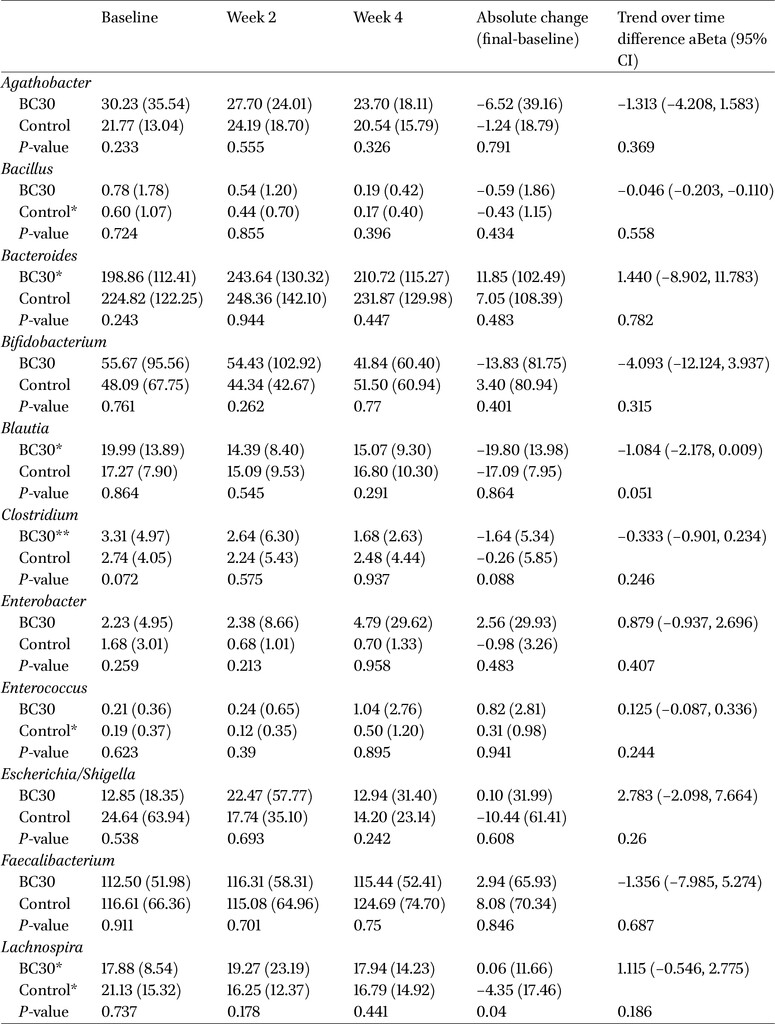
The abundance of different genera was also assessed and the most abundant genera across groups and visits were Bacteroides (average relative abundance: 22.6%), Faecalibacterium (11.7%), Prevotella (8.9%), Bifidobacterium (4.9%) and Agathobacter (2.5%), as shown in Figure 4. Average abundance of Bacillus genus was 0.05%, ranging from 0.074% at baseline to 0.02% at Week 4. A reduction in Bacillus species was observable in both study groups, although it was significant only in the control group (Friedmanâs test
Finally, Prevotella was shown to increase in both groups (Friedmanâs test
Despite the limited capability of V3/V4 16S RNA sequencing to accurately classify OTUs at the species level, we detected Heyndrickxia (Bacillus) coagulans in 16.1% and 14.5% of the samples from the BC30 and control groups, respectively, at baseline. At the end of the study, H. coagulans was detected in 7.3% of the samples from the BC30 group and 10.7% of the samples from the control group, although these differences were not statistically significant (
Alpha diversity indices comparing BC30 and control groups by time in study.
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
Relative abundance of detected genera comparing BC30 and control groups by time in the study.
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
Secondary outcomes
There were no significant differences in any of the eight physical and mental domains for quality of life, measured by the SF-36 questionnaires, for both the control group and the BC30 group (Supplementary Table S4).
Safety
Safety was assessed before and after the study interventions were given and the routine blood, urine and stool parameters and blood biochemical indexes were all within normal ranges (Supplementary Table S5). Participants in the intervention group reported a total of six adverse events (AEs), including nausea (
4 Discussion and conclusions
Our trial documented a significant improvement in gastrointestinal functions in healthy adults with impaired fecal excretion after 4 weeks of H. coagulans GBI-30, 6086 (BC30). In addition, BC30 was well tolerated by the participants. Significant improvements were found for an increase in the number of bowel movements/week, the absence of constipation and improvements in fecal consistency. In addition, improvements in intestinal functioning scores were found in the BC30 group compared with the control groups, including improved total GSRS score and improved scores for abdominal pain and constipation. The ability of BC30 to improve diverse GI symptoms may be due to the existence of multiple mechanisms of action inherent in living probiotics. BC30 may improve constipation by its ability to modulate intestinal microbiota, enhance gastrointestinal motility, increase water absorption and increase short-chain fatty acids via bile acid fermentation (Jager et al., 2018; Li et al., 2022; Nyangale et al., 2014, 2015; Steckler et al., 2020). BC30 may improve diarrhoea by competing with intestinal pathogens, reducing osmotic diarrhoea, and regulating immune responses (Anaya-Loyola et al., 2019; Dolin, 2009; Hun, 2009; Fitzpatrick et al., 2011; Gepner et al., 2017; Yang et al., 2014)
The introduction or removal of certain bacteria can lead to shifts in the microbial community due to competition for resources and space. Ingestion of BC30 influenced the abundance of several genera of intestinal normal microbiome (including Enterobacter spp. and Clostridium spp., for example) but did not dramatically affect the majority of other bacterial species in the intestine. BC30 also did not affect the diversity of types of bacteria found in the intestinal microbiome. This result is not unexpected, as the study population was generally healthy and their initial microbiome composition was already highly diverse. Alpha diversity may not have been affected in this population for many reasons: individual immune responses or use of antibiotics (not controlled in the study), not enough time to promote a shift in microbiome diversity, interactions of BC30 with the existing intestinal species, measurement and methodological variations, natural dynamics of microbiome populations, influence of diet, stress or other lifestyle factors. The lower carriage rate of Heyndrickxia (Bacillus) coagulans by the end of the study may reflect modulation in the microbiota rather than the change in absolute numbers due to changes in the diet that were not documented in the participantâs daily diaries. Additionally, the oral dosage of H. coagulans BC30 was 1Â Ã 109/day, which may have been below the detection level in the faeces using the methods employed.
Few clinical trials with this strain of bacteria have been published for functional intestinal disorders in healthy adults or children. Kalman et al. conducted a randomised, double-blinded trial in 61 adults with post-prandial intestinal gas-related symptoms who had no gastrointestinal diagnoses for their condition (Kalman et al., 2009). Participants were randomised to either B. coagulans GBI-30, 6086 (2Â Ã 109/capsule) or placebo for four weeks. No significant decrease in bloating or gas symptoms were found between the two groups. However, there was a significant improvement in total GSRS score and abdominal pain scores, similar to the results found in our trial. Although the population in this study and the formulations used differed from our trial, improvement in functional intestinal symptoms by BC30 were found in both studies. As the study by Kalman et al. was conducted in Miami, Florida and the Dominican Republic, the study population also differed by type of diet and other life-style characteristics (Kalman et al., 2009). A prospective, randomised trial by Kumar et al. (2020b) with B. coagulans GBI-30, 6086 enrolled elderly (55-75 years old) adults in India with indigestion and found a significant improvement in dyspepsia, abdominal pain and flatulence compared to placebo controls. Three meta-analyses found other strains of probiotics (L. casei Shirota and L. casei YIT9029) to be effective for improving chronic idiopathic constipation (Ford et al., 2014b; Kaminski et al., 2020; Zhang et al., 2020) but did not include any trials with H. coagulans GBI-30, 6086.
Other studies also examined the safety of BC30 and reported it is well tolerated. In one study of 50 elderly adults complaining of ingestion who were randomised B. coagulans GB-I30, 6086 or placebo, no significant differences in the frequency of mild reported adverse events (headache, nausea, vomiting, myalgia) were found in the BC30 group compared with the placebo group (24% and 32%, respectively) (Kumar et al., 2020b). Safety was also assessed using genomic procedures and phenotypic assays and found B. coagulans GBI-30, 6086 was resistant to streptomycin and kanamycin and no easily transferrable antibiotic-resistant genes or virulence factor genes were detected (Salvetti et al., 2016). In our trial, we also found there were no reported adverse reactions or significant changes in blood, stool or urine parameters.
Relative abundance of designated microorganisms in the BC30 group (
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00084
The strengths of this trial included a blinded, prospective, placebo-controlled study design to reduce potential biases of outcome assessments. Few randomised trials have focused on probiotic use in generally healthy adult populations, yet this is an increasingly common use for probiotics by the general population (Bodke et al., 2022; Sanders et al., 2018). We used a variety of standard and validated outcome measurements to capture changes in diverse GI tract symptoms present in the study population and assessed the impact of BC30 in the intestinal microbiome.
Limitations of this trial included the diversity of GI tract complaints in our enrolled population, which was a challenge to analyse but reflected the types of distress reported by the general population. Another limitation was the lack of follow-up after the study interventions were stopped. As diet was not tightly controlled during the study, participants may have taken excluded medications or dietary supplements during the study and failed to report this in their diaries.
While most studies finding significant efficacy of specific types of probiotics to improve GI tract symptoms and quality of life have been conducted in study populations with more severe disease (such as IBS) (Ceccherini et al., 2022; McFarland et al., 2021; Wen et al., 2020), our trial was conducted in the population with milder GI tract complaints. Thus, it may not be surprising that outcome measures developed to detect improvements in more severe diagnoses did not show significant improvements in our trial. For example, no significant improvement in the quality-of-life scores was found, but most study participants had high quality of life on enrollment. The results of this trial should only be generalised to healthy adults, with a caveat that nutritional and life-style differences in other geographic regions may alter the efficacy of BC30. In addition, more women were enrolled in our study than men, thus caution should be taken when extrapolating the efficacy to men, but in general, constipation and other GI complaints are more commonly reported in women globally (Bassotti et al., 2021; Black et al., 2018).
The role of probiotics has expanded from an adjunctive therapy in patients with existing disease or as a preventive strategy in high-risk patients to a broader role of improving health and functioning in generally healthy people. The implication for clinical practise and policy is that physicians and healthcare professionals should be aware that recommendations on the use of probiotics may differ in these two settings. More clinical trials in the future are needed in generally healthy populations to investigate specific strains of probiotics for clearly defined outcomes and to thoroughly assess safety. In addition, future trials should add a follow-up period after probiotics are discontinued to measure the stability of the effect and to detect any delayed onset adverse events.
Heyndrickxia (Bacillus) coagulans GBI-30, 6086 (BC30) significantly improved GI functions over four weeks of the intervention in healthy Chinese adults with minor modulations of the intestinal microbiome and was well-tolerated.
Corresponding author; e-mail:Â mcfarland.lynne.v@gmail.com
Acknowledgements
The authors would like to thank Intertek China and Intertek Canada and Beijing Hospital for their supervision of the trial and Beijing Novogene Technology Co., Ltd for microbiota analyses. Funding was provided by Kerry (Shanghai) Inc.
Authorsâ contribution
Conceptualisation: HG, JW. Data curation: HG, JW. Formal analysis: HG, JW, MES. Investigation: HG, JW. Methodology: HG, JW, MES, RB. Project administration: JW. Resources: HG, JW, MM. Supervision: HG, JW. Validation: RZ, MES, RB, MM. Visualisation: HG, JW, LVM. Writing â original draft: HG, JW, LVM. Writing â review and editing: HG, JW, LVM, RZ, MES, RB, MM. All authors have approved the submitted version of the manuscript.
Conflict of interest
The following authors are employed by Kerry Canada Inc. (RZ, MM) or Biosearch Life (MES, RB). LVM is a paid consultant to Kerry Inc. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Informed consent statement
A signed informed consent form was obtained from each enrolled participant.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki and approved on May 6, 2020 by the Ethnic Committee of Beijing Hospital, China (Approval # 2019BJYYEC-207-02).
References
Abhari, K., Saadati, S., Hosseini-Oskouiee, F., Yari, Z., Hosseini, H., Sohrab, G., Hejazi, E., Agah, S., Sadeghi, A. and Hekmatdoost, A., 2020. Is Bacillus coagulans supplementation plus low FODMAP diet superior to low FODMAP diet in irritable bowel syndrome management? European Journal of Nutrition 59: 2111-2117.
Adibpour, N., Hosseininezhad, M., Pahlevanlo, A. and Hussain, M.A., 2019. A review on Bacillus coagulans as a spore-forming probiotic. Applied Food Biotechnology 6(2): 91-100.
Altun, G.K. and Erginkaya, Z., 2021. Identification and characterization of Bacillus coagulans strains for probiotic activity and safety. Lebensmittel-Wissenschaft + Technologie 151: 112233. https://doi.org/10.1016/j.lwt.2021.112233
Anaya-Loyola, M.A., Enciso-Moreno, J.A., LoÌpez-Ramos, J.E., GarcıÌa-MarıÌn, G., AÌlvarez, M.Y., Vega-GarcıÌa, A.M., Mosqueda, J., GarcıÌa-GutieÌrrez, D.G., Keller, D. and PeÌrez-RamıÌrez, I.F., 2019. Bacillus coagulans GBI-30, 6068 decreases upper respiratory and gastrointestinal tract symptoms in healthy Mexican scholar-aged children by modulating immune-related proteins. Food Research International 125: 108567. https://doi.org/10.1016/j.foodres.2019.108567
Bassotti, G., Usai Satta, P. and Bellini, M., 2021. Chronic idiopathic constipation in adults: a review on current guidelines and emerging treatment options. Clinical and Experimental Gastroenterology 14: 413-428. https://doi.org/10.2147/CEG.S256364
Black, C.J. and Ford, A.C., 2018. Chronic idiopathic constipation in adults: epidemiology, pathophysiology, diagnosis and clinical management. Medical Journal of Australia 209: 86-91. https://doi.org/10.5694/mja18.0024
Black, C.J., Drossman, D.A., Talley, N.J., Ruddy, J. and Ford, A.C., 2020. Functional gastrointestinal disorders: advances in understanding and management. The Lancet 396: 1664-1674. https://doi.org/10.1016/S0140-6736(20)32115-2
Bodke, H. and Jogdand, S., 2022. Role of probiotics in human health. Cureus 14: e31313. https://doi.org/10.7759/cureus.31313
Cao, J., Yu, Z., Liu, W., Zhao, J., Zhang, H., Zhai, Q. and Chen, W., 2020. Probiotic characteristics of Bacillus coagulans and associated implications for human health and diseases. Journal of Functional Foods 64: 103643. https://doi.org/10.1016/j.jff.2019.103643
Caporaso, J.G., Kuczynski, J., Stombaugh, J., Bittinger, K., Bushman, F.D., Costello, E.K., Fierer, N., Pena, A.G., Goodrich, J.K., Gordon, J.I., Huttley, G.A., Kelley, S.T., Knights, D., Koenig, J.E., Ley, R.E., Lozupone, C.A., McDonald, D., Muegge, B.D., Pirrung, M., Reeder, J., Sevinsky, J.R., Turnbaugh, P.J., Walters, W.W., Widmann, J., Yatsunenko, T., Zaneveld, J. and Knight, R., 2010. QIIME allows analysis of high-throughput community sequencing data. Nature Methods 7: 335-336. https://doi.org/10.1038/nmeth.f.303
Ceccherini, C., Daniotti, S., Bearzi, C. and Re, I., 2022. Evaluating the efficacy of probiotics in IBS treatment using a systematic review of clinical trials and multi-criteria decision analysis. Nutrients 14: 2689. https://doi.org/10.3390/nu14132689
Chappidi, S., Villa, E.C. and Cantarel, B.L., 2019. Using Mothur to determine bacterial community composition and structure in 16S ribosomal RNA datasets. Current Protocols in Bioinformatics 67: e83. https://doi.org/10.1002/cpbi.83
Dolin, B.J., 2009. Effects of a proprietary Bacillus coagulans preparation on symptoms of diarrhea-predominant irritable bowel syndrome. Methods and Findings in Experimental and Clinical Pharmacology 31: 655-659. https://doi.org/10.1358/mf.2009.31.10.1441078
Dutta, P., Mitra, U., Dutta, S., Rajendran, K., Saha, T.K. and Chatterjee, M.K., 2011. Randomised controlled clinical trial of Lactobacillus sporogenes (Bacillus coagulans), used as probiotic in clinical practice, on acute watery diarrhoea in children. Tropical Medicine and International Health 16: 555-561. https://doi.org/10.1111/j.1365-3156.2011.02745.x
Edgar, R.C., Haas, B.J., Clemente, J.C., Quince, C. and Knight, R., 2011. UCHIME improves sensitivity and speed of chimera detection. Bioinformatics 27: 2194-2200. https://doi.org/10.1093/bioinformatics/btr381
Endres, J.R., Clewell, A., Jade, K.A., Farber, T., Hauswirth, J. and Schauss, A.G., 2009. Safety assessment of a proprietary preparation of a novel probiotic, Bacillus coagulans, as a food ingredient. Food and Chemical Toxicology 47: 1231-1238. https://doi.org/10.1016/j.fct.2009.02.018
Fan, H., Gao, L., Yin, Z., Ye, S., Zhao, H. and Peng, Q., 2022. Probiotics and rifaximin for the prevention of travelersâ diarrhea: a systematic review and network meta-analysis. Medicine 101: e30921. https://doi.org/0.1097/MD.000000000003092
Fijan, S., Fijan, T. and Conni, N., 2023. Overview of probiotic strains of Weizmannia coagulans, previously known as Bacillus coagulans, as food supplements and their use in human health. Applied Microbiology 3: 935-947. https://doi.org/10.3390/applmicrobiol3030064
Fitzpatrick, L.R., Small, J.S., Greene, W.H., Karpa, K.D. and Keller, D., 2011. Bacillus coagulans GBI-30 (BC30) improves indices of Clostridium difficile-induced colitis in mice. Gut Pathogens 3: 1-9. https://doi.org/10.1186/1757-4749-3-16
Ford, A.C., Mahadeva, S., Carbone, M.F., Lacy, B.E. and Talley, N.J., 2020. Functional dyspepsia. The Lancet 396: 1689-1702. https://doi.org/10.1016/S0140-6736(20)30469-4
Ford, A.C., Moayyedi, P., Lacy, B.E., Lembo, A.J., Saito, Y.A., Schiller, L.R., Soffer, E.E., Spiege, B.M. and Quigley, E.M., 2014a. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. American Journal of Gastroenterology 109: S2-S26. https://doi.org/10.1038/ajg.2014.187
Ford, A.C., Quigley, E.M.M., Lacy, B.E., Lembo, A.J., Sait, Y.A., Schiller, L.R., Soffer, E.E., Spiegel, M.R. and Moayyedi, P., 2014b. Efficacy of prebiotics, probiotics, and synbiotics in irritable bowel syndrome and chronic idiopathic constipation: systematic review and meta-analysis. American Journal of Gastroenterology 109: 1547-1561. https://doi.org/10.1038/ajg.2014.202
Gepner, Y., Hoffman, J.R., Shemesh, E., Stout, J.R., Church, D.D., Varanoske, A.N., Zelicha, H., Shelef, I., Chen, Y., Frankel, H. and Ostfeld, I., 2017. Combined effect of Bacillus coagulans GBI-30, 6086 and HMB supplementation on muscle integrity and cytokine response during intense military training. Journal of Applied Physiology 123: 11-18. https://doi.org/10.1152/japplphysiol.01116.2016
Guglielmetti, S., Mora, D., Gschwender, M. and Popp, K., 2011. Randomised clinical trial: Bifidobacterium bifidum MIMBb75 significantly alleviates irritable bowel syndrome and improves quality of life â a double-blind, placebo-controlled study. Alimentary Pharmacology and Therapeutics 33: 1123-1132. https://doi.org/10.1111/j.1365-2036.2011.04633.x
Hun, L., 2009. Bacillus coagulans significantly improved abdominal pain and bloating in patients with IBS. Postgraduate Medicine 121: 119-124. https://doi.org/10.3810/pgm.2009.03.1984
Jäger, R., Purpura, M., Farmer, S., Cash, H.A. and Keller, D., 2018. Probiotic Bacillus coagulans GBI-30, 6086 improves protein absorption and utilization. Probiotics and Antimicrobial Proteins 10: 611-615. https://doi.org/10.1007/s12602-017-9354-y
Kalman, D.S., Schwartz, H.I., Alvarez, P., Feldman, S., Pezzullo, J.C. and Krieger, D.R., 2009. A prospective, randomized, double-blind, placebo-controlled parallel-group dual site trial to evaluate the effects of a Bacillus coagulans-based product on functional intestinal gas symptoms. BMC Gastroenterology 9: 1-7. https://doi.org/10.1186/1471-230X-9-85
KaminÌski, M., Skonieczna-ZÌydecka, K., Åoniewski, I., Koulaouzidis, A. and Marlicz, W., 2020. Are probiotics useful in the treatment of chronic idiopathic constipation in adults? A review of existing systematic reviews, meta-analyses, and recommendations. Gastroenterology Review 15: 103-118. https://doi.org/10.5114/pg.2019.86747
Keller, D., Verbruggen, S., Cash, H., Farmer, S. and Venema, K., 2019. Spores of Bacillus coagulans GBI-30, 6086 show high germination, survival and enzyme activity in a dynamic, computer-controlled in vitro model of the gastrointestinal tract. Beneficial Microbes 10: 77-87. https://doi.org/10.3920/BM2018.0037
Kulich, K.R., Madisch, A., Pacini, F., PiqueÌ, J.M., Regular, J., Van Rensburg, C.J., UÌjszaÌszy, L., Carlsson, J., Halling, K. and Wiklund, I.K., 2008. Reliability and validity of the gastrointestinal symptom rating scale (GSRS) and quality of life in reflux and dyspepsia (QOLRAD) questionnaire in dyspepsia: a six country study. Health Quality and Life Outputs 6: 12. https://doi.org/10.1186/1477-7525-6-12
Kumar, R., Sood, U., Gupta, V., Singh, M., Scaria, J. and Lal, R., 2020a. Recent advancements in the development of modern probiotics for restoring human gut microbiome dysbiosis. Indian Journal of Microbiology 60: 12-25.
Kumar, V.V., Sudha, K.M., Bennur, S. and Dhanasekar, K.R., 2020b. A prospective, randomized, open-label, placebo-controlled comparative study of Bacillus coagulans GBI-30, 6086 with digestive enzymes in improving indigestion in geriatric population. Journal of Family Medicine Primary Care 9: 1108-1112. https://doi.org/10.4103/jfmpc.jfmpc_922_19
Li, L., Liu, B., Cao, J., Zhang, H., Tian, F., Yu, L., Chen, W. and Zhai, Q., 2022. Different effects of Bacillus coagulans vegetative cells and spore isolates on constipation-induced gut microbiota dysbiosis in mice. Food & Function 13(18): 9645-9657.
Madempudi, R.S., Neelamraju, J., Ahire, J.J., Gupta, S.K. and Shukla, V.K., 2020. Bacillus coagulans unique IS2 in constipation: a double-blind, placebo-controlled study. Probiotics and Antimicrobial Proteins 12: 335-342. https://doi.org/10.1007/s12602-019-09542-9
MagocÌ, T. and Salzberg, S.L., 2011. FLASH: fast length adjustment of short reads to improve genome assemblies. Bioinformatics 27: 2957-2963. https://doi.org/10.1093/bioinformatics/btr507
Majeed, M., Nagabhushanam, K., Paulose, S., Arumugam, S. and Mundkur, L., 2023. The effects of Bacillus coagulans MTCC 5856 on functional gas and bloating in adults: a randomized, double blind, placebo-controlled study. Medicine 102: e33109. https://doi.org/10.1097/MD.0000000000033109
McFarland, L.V., Evans, C.T. and Goldstein, E.J., 2018. Strain-specificity and disease-specificity of probiotic efficacy: a systematic review and meta-analysis. Frontiers in Medicine 5: 124. https://doi.org/10.3389/fmed.2018.00124
McFarland, L.V., Karakan, T. and Karatas, A., 2021. Strain-specific and outcome-specific efficacy of probiotics for the treatment of irritable bowel syndrome: a systematic review and meta-analysis. eClinicalMedicine 41: 101154. https://doi.org/10.1016/j.eclinm.2021.101154
Merenstein, D.J., Tancredi, D.J., Karl, J.P., Krist, A.H., Lenoir-Wijnkoop, I., Reid, G., Roos, S., Szajewska, H. and Sanders, M.E., 2024. Is there evidence to support probiotic use for healthy people? Advances in Nutrition 15: 100265. https://doi.org/10.1016/j.advnut.2024.100265
Ministry of Health of the Peopleâs Republic of China, 2003. Technical standards for testing & assessment of health food. China Bureau of Scientific Standards, Standards Press of China/Ministry of Health of the Peopleâs Republic of China, Beijing, Peopleâs Republic of China, pp. 148-153.
Moher, D., Hopewell, S., Schulz, K.F., Montori, V., Gøtzsche, P.C., Devereaux, P.J., Elbourne, D., Egger, M. and Altman, D.G., 2010. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. British Medical Journal 340: c869. https://doi.org/10.1136/bmj.c869
Narsing Rao, M.P., Banerjee, A., Liu, G.H. and Thamchaipenet, A., 2023. Genome-based reclassification of Bacillus acidicola, Bacillus pervagus and the genera Heyndrickxia, Margalitia and Weizmannia. International Journal of Systematic and Evolutionary Microbiology 73: 005961. https://doi.org/10.1099/ijsem.0.005961
Nyangale, E.P., Farmer, S., Cash, H.A., Keller, D., Chernoff, D. and Gibson, G.R., 2015. Bacillus coagulans GBI-30, 6086 modulates Faecalibacterium prausnitzii in older men and women. The Journal of Nutrition 145: 1446-1452. https://doi.org/10.3945/jn.114.199802
Nyangale, E.P., Farmer, S., Keller, D., Chernoff, D. and Gibson, G.R., 2014. Effect of prebiotics on the fecal microbiota of elderly volunteers after dietary supplementation of Bacillus coagulans GBI-30, 6086. Anaerobe 30: 75-81. https://doi.org/10.1016/j.anaerobe.2014.09.002
Rabeneck, L., 2003. Measuring dyspepsia-related health in randomized trials: the Severity of Dyspepsia Assessment (SODA) and its use in treatment with NSAIDs and COX-2-specific inhibitors. Rheumatology 42: iii32-9. https://doi.org//10.1093/rheumatology/keg496
Rathi, A. and Pagare, R., 2024. Efficacy and safety of Bacillus coagulans LBSC in drug induced constipation associated with functional gastrointestinal disorder: a double-blind, randomized, interventional, parallel, controlled trial a clinical study. Global Advances in Integrative Medicine and Health 13: 1-19. https://doi.org/10.1177/27536130241286511
Revicki, D.A., Wood, M., Wiklund, I. and Crawley, J., 1997. Reliability and validity of the gastrointestinal symptom rating scale in patients with gastroesophageal reflux disease. Quality of Life Research 7: 75-83. https://doi.org/10.1023/A:1008841022998
Salvetti, E., OrruÌ, L., Capozzi, V., Martina, A., Lamontanara, A., Keller, D., Cash, H., Felis, G.E., Cattivelli, L., Torriani, S. and Spano, G., 2016. Integrate genome-based assessment of safety for probiotic strains: Bacillus coagulans GBI-30, 6086 as a case study. Applied Microbiology and Biotechnology 100: 4595-4605. https://doi.org/10.1007/s00253-016-7416-9
Sanders, M.E., Merenstein, D., Merrifield, C.A. and Hutkins, R., 2018. Probiotics for human use. Nutrition Bulletin 43: 212-225. https://doi.org/10.1111/nbu.12334
Saneian, H., Pourmoghaddas, Z., Roohafza, H. and Gholamrezaei, A., 2015. Synbiotic containing Bacillus coagulans and fructo-oligosaccharides for functional abdominal pain in children. Gastroenterology and Hepatology From Bed to Bench 8: 56-65.
Shin, A., Preidis, G.A., Shulman, R. and Kashyap, P.C., 2019. The gut microbiome in adult and pediatric functional gastrointestinal disorders. Clinical Gastroenterology and Hepatology 17: 256-274. https://doi.org/10.1016/j.cgh.2018.08.054
Sniffen, J.C., McFarland, L.V., Evans, C.T. and Goldstein, E.J.C., 2018. Choosing an appropriate probiotic product for your patient: an evidence-based practical guide. PLoS ONE 13: e0209205. https://doi.org/10.1371/journal.pone.0209205
Soares, M.B., Martinez, R.C., Pereira, E.P., Balthazar, C.F., Cruz, A.G., Ranadheera, C.S. and SantâAna, A.S., 2019. The resistance of Bacillus, Bifidobacterium, and Lactobacillus strains with claimed probiotic properties in different food matrices exposed to simulated gastrointestinal tract conditions. Food Research International 125: 108542. https://doi.org/10.1016/j.foodres.2019.108542
Stecker, R.A., Moon, J.M., Russo, T.J., Ratliff, K.M., Mumford, P.W., Jäger, R., Purpura, M. and Kerksick, C.M., 2020. Bacillus coagulans GBI-30, 6086 improves amino acid absorption from milk protein. Nutrition & Metabolism 17: 93. https://doi.org/10.1186/s12986-020-00515-2
Tian, H., Ge, X., Niey, Y., Yang, L., Ding, C., McFarland, L.V., Zhang, X., Chen, Q., Gong, J. and Li, N., 2017. Fecal microbiota transplantation in patients with slow-transit constipation: a randomized, clinical trial. PLoS ONE 12: e0171308. https://doi.org/10.1371/journal.pone.0171308
Tian, H., Chen, Q., Yang, B., Qin, H. and Li, N., 2021. Analysis of gut microbiome and metabolite characteristics in patients with slow transit constipation. Digestive Diseases and Sciences 66: 3026-3035. https://doi.org/10.1007/s10620-020-06500-2
Walden, K.E., Hagele, A.M., Orr, L.S., Gross, K.N., Krieger, J.M., Jäger, R. and Kerksick, C.M., 2024. Probiotic BC30 improves amino acid absorption from plant protein concentrate in older women. Probiotics and Antimicrobial Proteins 16: 125-137. https://doi.org/10.1007/s12602-022-10028-4
Ware Jr, J.E., 2000. SF-36 health survey update. Spine 25: 3130-3139.
Wen, Y., Li, J., Long, Q., Yue, C.C., He, B. and Tang, X.G., 2020. The efficacy and safety of probiotics for patients with constipation-predominant irritable bowel syndrome: a systematic review and meta-analysis based on seventeen randomized controlled trials. International Journal of Surgery 79: 111-119. https://doi.org/10.1016/j.ijsu.2020.04.063
Yang, O.O., Kelesidis, T., Cordova, R. and Khanlou, H., 2014. Immunomodulation of antiretroviral drug-suppressed chronic HIV-1 infection in an oral probiotic double-blind placebo-controlled trial. AIDS Research and Human Retroviruses 30: 988-995. https://doi.org/10.1089/aid.2014.0181
Yang, Y.X., He, M., Hu, G., Wei, J., Pages, P., Yang, X.H. and Bourdu-Naturel, S., 2008. Effect of a fermented milk containing Bifidobacterium lactis DN-173010 on Chinese constipated women. World Journal of Gastroenterology 14: 6237-6243. https://doi.org/10.3748/wjg.14.6237
Zhang, C., Jiang, J., Tian, F., Zhao, J., Zhang, H., Zhai, Q. and Chen, W., 2020. Meta-analysis of randomized controlled trials of the effects of probiotics on functional constipation in adults. Clinical Nutrition 39: 2960-2969. https://doi.org/10.1016/j.clnu.2020.01.005
Zou, G., Zou, L. and Qiu, S.F., 2023. Parametric and nonparametric methods for confidence intervals and sample size planning for win probability in parallel-group randomized trials with Likert item and Likert scale data. Pharmaceutical Statistics 22: 418-439. https://doi.org/10.1002/pst.2280





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}