Abstract
Antibiotics are among the most prescribed medicines in children globally. Antibiotic-associated diarrhoea (AAD) and associated abdominal pain are common side effects, caused by alterations to the intestinal microbiota composition. Most research on probiotic interventions involves prophylactic use of Saccharomyces, lactobacilli or bifidobacteria. Less is known about spore-forming strains administered after AAD onset. Bacillus subtilis HU58⢠was found to improve AAD symptoms in adults. This randomised, double-blind, placebo-controlled trial in India investigated the effects of a dietary supplement containing B. subtilis HU58 (2 à 109 cfu/day) versus placebo for seven days on diarrhoea duration (Bristol Stool Scale, BSS), abdominal pain intensity (Visual Analogue Scale, VAS), and overall gastrointestinal wellbeing (adapted Gastrointestinal Restoration Questionnaire, GIRQ; Physician Global Assessment, PGA) in 68 children (1-12 years) with AAD. Between-group comparison of data from each timepoint was conducted for the intention to treat population (Chi-squared test of independence for distribution of BSS types, Wilcoxon rank sum test for mean BSS types, mixed model for repeated measures for VAS, GIRQ and PGA scores). By day 3, 93.5% of the probiotic group had normal BSS types, versus 22.6% in the placebo group (
The trial is registered at https://ctri.nic.in/Clinicaltrials (CTRI/2022/02/040138).
1 Introduction
The burden of infectious disease is high, particularly in developing countries such as India, and studies have shown antibiotics to be among the most prescribed drug classes for paediatric populations in this region (Karande et al., 2005; Kumar et al., 2008). Whilst necessary for the treatment of bacterial infections in some cases, antibiotics have several known side effects (Singh et al., 2014), with antibiotic-associated diarrhoea (AAD) recognised as one of the most common. AAD may affect up to 40% of children receiving broad-spectrum antibiotic treatment globally (Guo et al., 2019), with the highest prevalence reported for antibiotics which target anaerobes, such as aminopenicillins, cephalosporins and clindamycin (McFarland, 2008; Wiström et al., 2001). Left untreated, severe AAD may lead to electrolyte and fluid imbalances, pseudomembranous colitis, and life-threatening complications in rare cases (McFarland, 2008).
AAD is caused by the unintended disruption of the normal intestinal microbiota by antibiotic use, leading to opportunistic overgrowth of pathogens (commonly Clostridium difficile) and osmotic shifts within the bowel (Binder, 2010; Francino, 2015). AAD is characterized by the onset of loose stools at least three times per day, occurring a few hours up to a few weeks after antibiotic administration (McFarland, 2008), with concurrent abdominal pain or discomfort commonly reported (Guo et al., 2019).
The presence of AAD may reduce compliance rates to prescribed antibiotic therapy (BauÌ et al., 2020), with implications for the efficacy of treatment for the individual, and antimicrobial resistance more generally (World Health Organization (WHO), 2001). As such, effective management of side effects such as AAD and abdominal pain may be an important consideration for antimicrobial sustainability.
The use of probiotics to address the underlying gut microbiota disturbances for the prevention or management of AAD is well established. Several studies have demonstrated the safety and efficacy of probiotics in paediatric populations with AAD (Guo et al., 2019). To date, most clinical research in this area has investigated the effects of the prophylactic use of Saccharomyces, Lactobacillus or Bifidobacterium species for the prevention of AAD (Guo et al., 2019). Fewer studies have investigated the effects of other species administered therapeutically following the onset of AAD, particularly spore-forming bacterial strains which may offer additional benefits.
Spore-forming probiotic strains are of increasing interest for their human health applications, due to their ability to survive harsh conditions such as acidic environments and extreme temperatures. Compared to non-spore-formers, their stability may render them more viable during gut transit, manufacturing, and storage, particularly in warmer climates, thus enabling the versatility of various supplement formats to suit the diverse needs of different target populations (Soares et al., 2023).
The Bacillus subtilis HU58⢠strain was first isolated from a healthy human gut (Hong et al., 2009). Its safety profile has been confirmed by genome sequencing, clinical trials (Dhongade, 2022; Mehta, 2020a,b), with Qualified Presumption of Safety (QPS) and Generally Recognized as Safe (GRAS) certification (Dound, 2017). Previous clinical findings have demonstrated that this spore-forming probiotic improves stool consistency and frequency in adults with AAD (Mehta, 2020b). When administered in combination with Bacillus coagulans SC208®, B. subtilis HU58 was found to improve stool consistency and reduce duration of diarrhoea in adults with AAD (Mehta, 2020a) and children with both infectious diarrhoea and AAD (Dhongade, 2022). However, less is known about the effects of this spore-forming probiotic strain alone on the gastrointestinal symptoms of children with AAD.
This double-blind, randomised, placebo-controlled trial was conducted in India to investigate the effect of a dietary supplement containing B. subtilis HU58, on the duration of diarrhoea, the intensity of abdominal pain, and overall GI wellbeing, in children with AAD.
2 Materials and methods
Study subjects
Children who presented to the Dr Pramod Jog Childrenâs Clinic or Mankar Hospital in India with AAD were screened for study recruitment. Children were eligible for inclusion if they were aged one to 12 years, with an onset of AAD (defined as passage of three or more liquid or watery stools in a 24-hour period) within two to three days of initiating antibiotic therapy (any type, for any indication), with willingness of both the parent/guardian and the child to participate in the study and to provide informed consent (and assent from the child, where possible). Exclusion criteria were: (i) history of pre-existing diarrhoea within the previous four weeks, functional diarrhoea/constipation, inflammatory bowel disease, malabsorption syndrome or other GI disorder, bowel carcinoma, symptoms or suspicion of organic lesion of the digestive tract, undiagnosed abdominal pain or rectal bleeding, gastrointestinal surgery, severe chronic systemic disease, critical/life-threatening illness or immunodeficiency diseases, bloody and/or purulent stools, severe dehydration requiring intravenous rehydration, lactose intolerance, known hypersensitivity to any ingredients of the study product or placebo, or any other condition deemed by the investigator to contraindicate participation; (ii) use of proton-pump inhibitors, laxatives, anti-diarrhoeal drugs or probiotics within 14 days prior to and/or during the study; (iii) children requiring hospitalisation; and (iv) participation in another clinical study within 30 days prior to and/or during this clinical study.
Ethical considerations
Participation in the study was voluntary. Written informed consent was obtained for all subjects by their parent/guardian, who was informed that they could withdraw their child from the study at any time. The study protocol was approved by the Independent Ethics Committee of Dhanashree Hospital, Pune, India (Permission No. IECDH/2022/02 dated 7th July 2022).
The trial was conducted in accordance with relevant health-related research guidelines of the Indian Ministry of Health and Family Welfare and the Indian Council of Medical Research, the International Conference for Harmonisationâs guideline for Good Clinical Practice, and the Declaration of Helsinki.
The trial was prospectively registered in the Clinical Trial Registry of India (CTRI/2022/02/040138). Consolidated Standards of Reporting Trials (CONSORT) guidelines were followed for reporting trial results.
Study materials
Eligible subjects were recruited into the study and randomly allocated to one of two subgroups to receive either a probiotic syrup (B. subtilis HU58 [2Â Ã 109 colony-forming units (CFU) per vial], sugar, water, dispersing agent [INS 1520], color [INS 129], mixed fruit flavor, preservatives [INS 129, 217]) or a placebo syrup without the probiotic, manufactured by Synergia Life Sciences (formerly known as Riata Life Sciences) Pvt Ltd, Vadodara, India. The probiotic and placebo syrups had a similar appearance, taste, and smell and were packed in identical single-dose 5Â ml vials.
Randomisation and blinding
The randomisation list was generated by a person not directly involved in the study. Randomisation to the two groups was performed in a 1:1 ratio in blocks of eight. Study products were labelled according to the randomisation lists and only identifiable by the randomisation number. Allocation was performed by the investigator in consecutive order by assigning each eligible subject the first available randomisation number for the relevant group. Subjects, parents/guardians, investigators, and clinical staff involved in the study were blinded until the final database was locked.
Study protocol
Subjects consumed one vial of the probiotic or placebo syrup three hours after administration of their antibiotic, once a day for seven days. Clinical evaluation was performed during three in-person study visits. Visit 1 was a screening/baseline visit on day 0 followed by study visits on day 3 (visit 2) and 7 (visit 3), where outcome measurements were assessed by the investigator. Subject compliance to the study products was assessed by study site personnel, who measured the amount of study products returned at the end of the study versus the amount dispensed to each subject.
Outcome measures
The primary outcome was stool consistency, assessed using the Bristol Stool Scale (BSS) (Lewis and Heaton, 1997). The BSS classifies stool into seven categories: types 1-2 (constipated), types 3-5 (normal), and types 6-7 (loose stool-diarrhoea). Secondary outcomes included abdominal pain intensity, general GI wellbeing, and safety. Abdominal pain intensity was assessed using a 10Â cm Visual Analogue Scale (VAS) adapted to ask parents/participants to indicate their pain intensity from 0 (least pain) to 10 (most pain) (Gallagher et al., 2002). Simple language was used to support understanding of the scale and communication of the childâs pain intensity. For younger children, parents assessed pain intensity by observing the childâs behaviour, body language, movements and facial expressions. General gastrointestinal health was assessed with an adapted Gastrointestinal Restoration Questionnaire (GIRQ) (Porter et al., 2020) and a physician global assessment (PGA).
The adapted questionnaire included 30 questions from the GIRQ (scored from 0 [almost never] to 3 [most of the time/severe]) relating to various aspects of GI health such as abdominal pain, bloating, fullness, belching, appetite, bowel habits, flatulence, nausea/vomiting and food sensitivities, omitting questions from the original tool relating to other holistic aspects such as micronutrient status, headaches, skin rashes, etc. Scores were then accumulated into a composite score, with a maximum of 70 points indicating greatest symptom severity. Additionally, the PGA used a 10-point scale (1 very poor to 10 excellent) to assess perception of the subjectâs gastrointestinal health overall.
Safety was assessed by occurrence of adverse events (AEs) throughout the study.
Sample size calculation
Based on previously published data on the effects of this B. subtilis HU58 in adults with AAD (Mehta, 2020b), in the present study, the mean BSS score on Day 7 was expected to be four and seven in the probiotic and placebo groups, respectively. Considering the common standard deviation as two, two-sided level of significance as 5%, randomisation ratio as 1:1 and power as 99%, it was determined that the study would need at least 52 evaluable subjects (completed cases) with 26 subjects in each arm, requiring recruitment of 69 subjects to allow for a 25% drop-out rate.
Statistical analysis
Data are presented as mean (standard deviation, SD) and proportion (n, %) of subjects, unless otherwise stated. Statistical analysis was performed using SPSS version 22.0 (IBM, Armonk, USA) on all available data from the intention to treat (ITT) population (those who consumed at least one vial of the allocated study product) with omission of missing data. Between-group differences in the distribution of BSS stool types at each time point were analysed with the Chi-squared test of independence, comparing the proportion of subjects with each BSS subtype in each group. A non-parametric Wilcoxon rank sum test was applied to compare the mean BSS stool types between the groups at each visit, due to abnormal distribution of this data. Between-group differences in VAS, GIRQ and PGA scores at each timepoint were analysed using a mixed model for repeated measures. A P value of <0.05 was considered statistically significant.
3 Results
Subjects
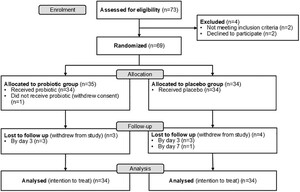
In total, 73 children were screened and 69 were enrolled into the study, following two screen failures and two subjectsâ parents/guardians withdrawing consent before randomisation. During the intervention phase, 69 subjects were randomised to receive the probiotic (n = 35) or placebo (n = 34). One subject in the probiotic group withdrew from the study before administration of the study product, leaving 34 in each group at baseline. Seven subjects were lost to follow up (n = 3 probiotic group; n = 4 placebo group) (Figure 1).

CONSORT flow diagram of study.
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00086
Baseline characteristics
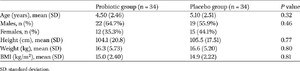
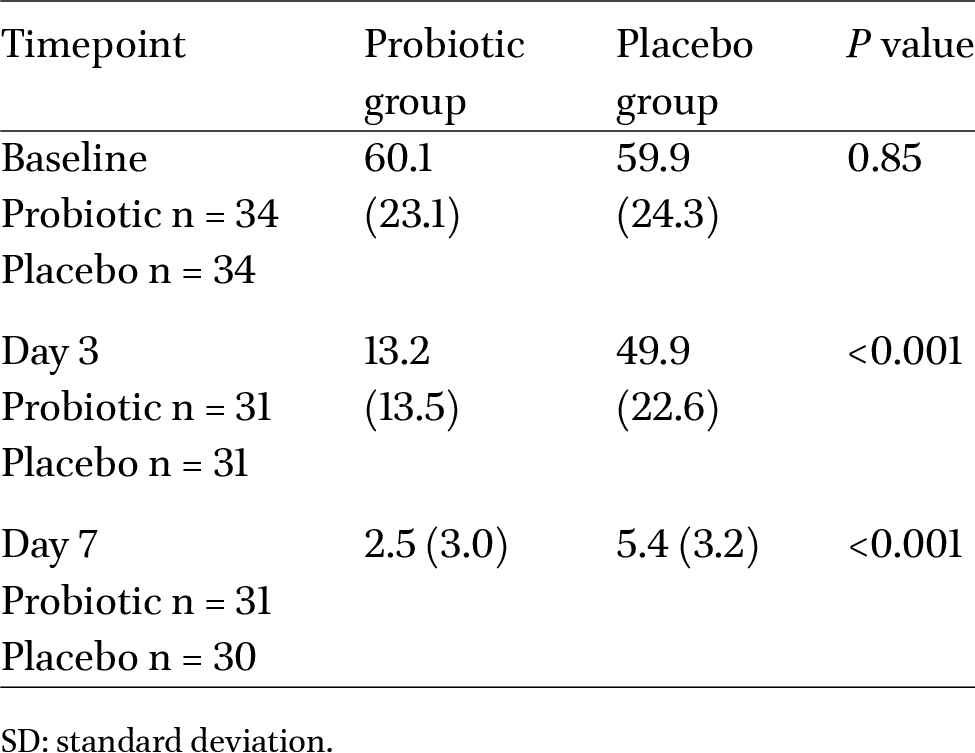
At baseline, subjects were prescribed standard paediatric dosages of a range of antibiotics, namely β-lactam antibiotics including penicillins (amoxicillin with or without a β-Lactamase inhibitor, 35.3%) and cephalosporins (cefixime, 30.9%; cefpodoxime with or without a β-Lactamase inhibitor, 13.2%; cefalexin, 2.9%); macrolides (azithromycin, 14.7%); fluoroquinolone (ofloxacin 1.5%); and a combination of fluoroquinolone and nitroimidazole (ofloxacin and metronidazole, 1.5%), with no significant differences between groups (
Summary of subject demographic characteristics at baseline
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00086
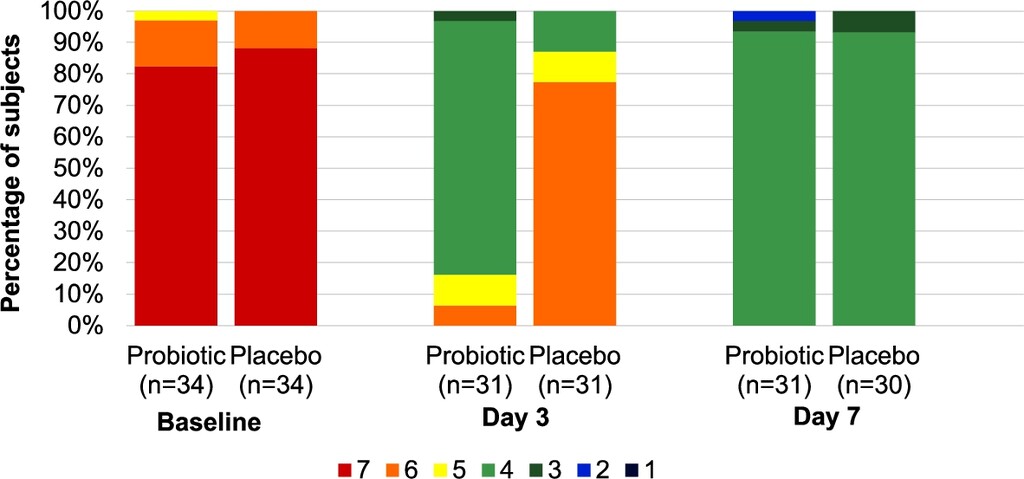
Percentage of subjects with each Bristol Stool Scale (BSS) type in probiotic versus placebo groups at each timepoint. Differences in the distribution of stool types between groups was statistically significant at day 3 (
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00086
Response to probiotic
Bristol Stool Scale (BSS)
At baseline, stool consistency was categorized as diarrhoea (type 6 or 7) for all but one subject (type 5; n = 1 in probiotic group), with no significant differences between groups (
Similar trends were observed in the mean BSS scores at each timepoint, with similar scores between groups at baseline (probiotic group 6.79 [SD 0.48]; placebo group 6.88 [SD 0.33],
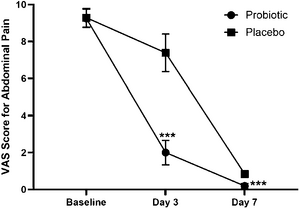
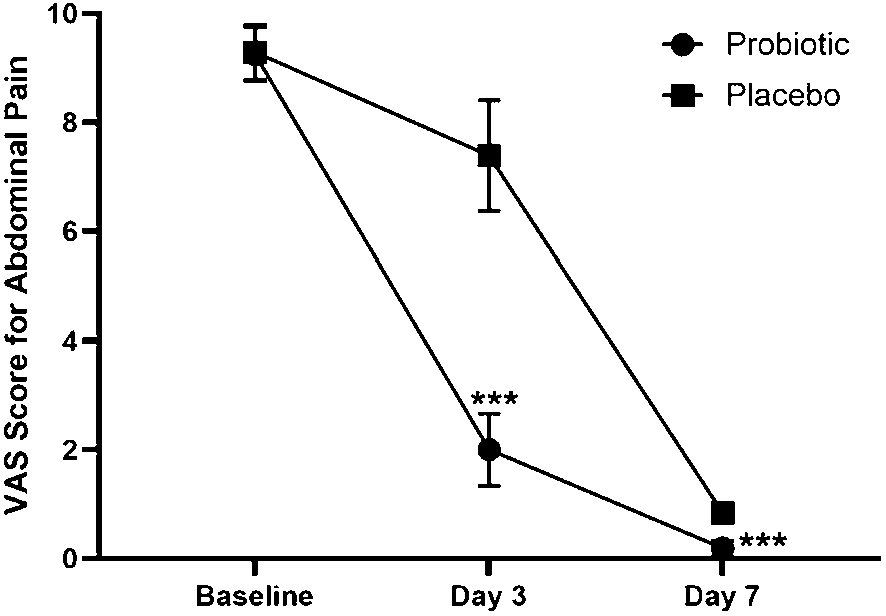
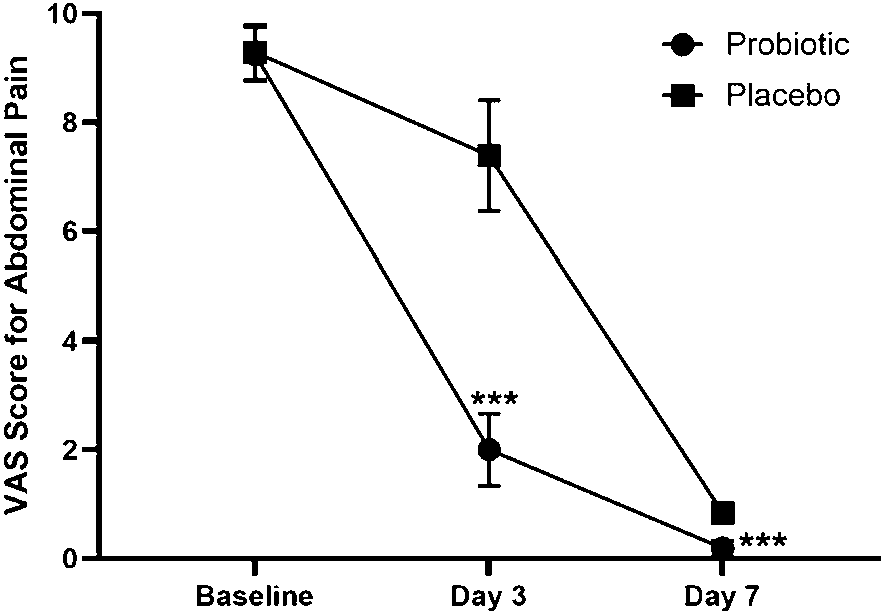
Visual Analogue Scale (VAS)
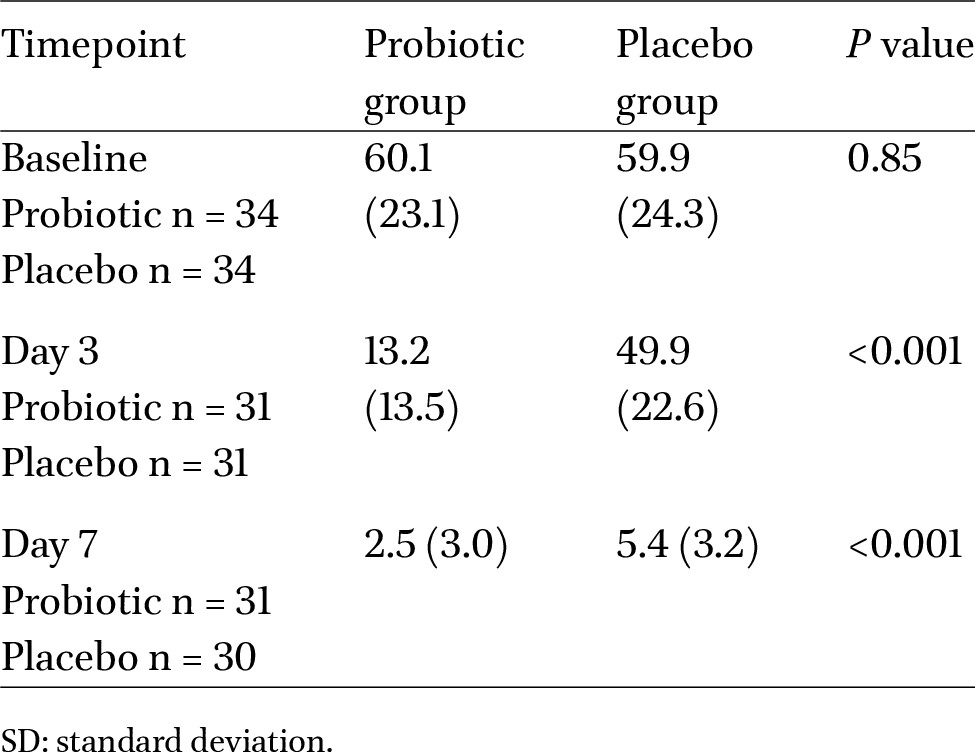
At baseline, there was no statistically significant difference in VAS score for abdominal pain intensity between groups (
Mean (SD) Visual Analogue Scale (VAS) score for abdominal pain intensity in probiotic versus placebo groups at each timepoint. ***
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00086
Gastrointestinal Restoration Questionnaire (GIRQ)
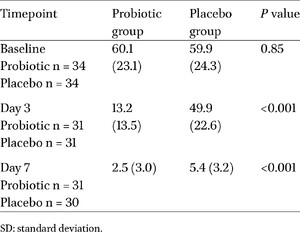
Mean composite GIRQ scores for general GI wellbeing were similar at baseline, with no significant differences between groups. During the study period, the decrease in mean composite GIRQ score was significantly greater in the probiotic group (Table 2).
Mean composite Gastrointestinal Restoration Questionnaire (GIRQ) score for abdominal wellbeing in probiotic versus placebo groups at each timepoint
Citation: Beneficial Microbes 17, 1 (2026) ; 10.1163/18762891-bja00086
Physician Global Assessment (PGA)
There was no statistically significant difference in PGA scores for general GI wellbeing between the probiotic and placebo groups at baseline (1.5 [SD 1.2] versus 1.8 [SD 1.8], respectively,
Safety (adverse events)
During the study, two AEs (excessive vomiting) were recorded (n = 1 probiotic group; n = 1 placebo group). These were both categorized as moderate severity and unlikely to be related to use of the study products.
Study product compliance
During the intervention period, mean compliance with the study product was high and similar between groups (97.1% of dispensed product consumed in the probiotic group versus 98.1% in the placebo group).
4 Discussion
The results of this randomised, double-blind, placebo-controlled trial showed that a dietary supplement containing B. subtilis HU58 was safe and well tolerated, with excellent rates of compliance, leading to a significantly faster resolution of diarrhoea, greater reduction in abdominal pain intensity, and significant improvements in general GI wellbeing compared to placebo, in children with AAD.
Antibiotic usage is increasing globally, and India has the second highest overall antibiotic consumption in the world, with a 47% increase from 2010 to 2020 (Mehta et al., 2022). A survey of parents of young children in India found that 16% of children had been prescribed four or more courses of antibiotics within the last year (Agarwal et al., 2015). The excessive use and misuse of antibiotics give rise to concerns about antimicrobial resistance, which directly causes over 300,000 deaths in India alone each year (Nogrady, 2023). In addition to overuse, nonadherence to prescribed treatment courses may further contribute to antimicrobial resistance (Kotwani et al., 2021; World Health Organization (WHO), 2001). With discomfort cited as a key reason for nonadherence (BauÌ et al., 2020; Endashaw Hareru et al., 2022), effective management of common side effects including AAD and associated abdominal pain may be of clinical importance.
In contrast to most studies which investigate the incidence of AAD following prophylactic use of probiotics (Yang et al., 2023), the present study demonstrated efficacy of B. subtilis HU58 administered within two to three days following the onset of AAD, indicating a clinical role for probiotics beyond the immediate timeframe of antibiotic initiation. Whilst diarrhoea was resolved in all subjects within seven days, the administration of B. subtilis HU58 resulted in a faster resolution, with significantly more subjects experiencing normal stool types by day 3, compared to the placebo group. As outcomes were not measured daily, it was not possible to determine how soon the diarrhoea was resolved within this three-day period. Findings of recent systematic reviews have demonstrated that the use of probiotics led to a reduction of 0.6-1.95 days in the duration of AAD in children (Yang et al., 2023), with a significantly greater efficacy rate for the treatment of AAD at day 2, compared to placebo (Huang et al., 2021).
The observed improvement in diarrhoea in the present study was accompanied by significant reductions in abdominal pain and overall GI wellbeing, which were evident from day 3 to the end of the study period. These findings offer a broader insight into the efficacy of probiotics beyond the normalisation of stool consistency, and the overall patient experience of the management of paediatric AAD. However, to date, the reporting of the effects of probiotics on abdominal pain and related GI wellbeing outcomes in children with AAD is limited and has been recommended as a specific focus for future research (Huang et al., 2021).
The clinical improvements observed in the present study following the administration of B. subtilis HU58 may have been mediated, in part, by the immunoregulatory properties of this probiotic strain. It has been demonstrated that the HU58 strain interacts with toll-like receptors, stimulates the proliferation of cells within the gut-associated lymphoid tissue, and activates potent innate immune responses in a murine model (Huang et al., 2008). In addition, in vitro studies have indicated that spore forming Bacillus strains may enhance production of short-chain fatty acids such as butyrate, acetate, and propionate (Duysburgh et al., 2019), which may support intestinal epithelial barrier integrity by contributing to tight junction assembly, increasing mucin expression, and reducing intestinal inflammation (Priyadarshini et al., 2018). Indeed, daily administration of B. subtilis HU58 at a dose of 2 à 109 cfu over an 8-week period was shown to significantly decrease levels of proinflammatory cytokines, interleukin-6 and tumour necrosis factor-α, in healthy people (Dound, 2017).
The properties and effects of probiotics are strain specific, with some showing no clinical benefit in this area (Huang et al., 2021; Yang et al., 2023). The viability of B. subtilis HU58 as a spore-forming strain may support its potential to exert positive health effects upon the host (Soares et al., 2023). In addition, the stability of spores facilitates manufacturing, transportation and storage, particularly in diverse climates and challenging environmental conditions, enabling supplement availability in formats more suitable for certain populations, such as syrups or gummies for children, which may support compliance, but which may not be feasible with non-spore-forming strains requiring cold-chain production.
As probiotic microorganisms may not permanently colonize the gastrointestinal tract, consistent intake in adequate amounts is required for clinical efficacy (Goodman et al., 2021). In the present study, compliance to the probiotic regimen was found to be very high, at over 97%. Furthermore, the tolerability of B. subtilis HU58 was confirmed by the absence of AEs related to the study product, which was consistent with previously published findings (Dhongade, 2022; Mehta, 2020a,b). Typically, the incidence of adverse reactions to probiotics has been found to be low among children with AAD, indicating the general safety of their use in this population (Yang et al., 2023).
The present study has limitations that should be considered for future investigations. Daily clinical assessment of outcomes, including the frequency of bowel movements, using tools validated in the study population and an extended follow-up period, may have enabled more specific conclusions about the timescale of symptom resolution following probiotic administration. Analysis of faecal samples may have supported our understanding of the ability of this spore-forming bacterium to restore gut microbiota composition following antibiotic use, and would have offered insights into several mechanisms ascribed to the B. subtilis species (Rhayat et al., 2019) and possibly AAD in general. Whilst variation in the type, duration and clinical indication of antibiotic prescriptions introduced heterogeneity among the study cohort, this may offer some indication of the spectrum of effectiveness of this strain in real-world populations. Future studies comparing the effects of B. subtilis HU58 with other probiotic strains commonly used in the management of AAD would also be warranted. Despite its limitations, this is the first study to demonstrate the clinical efficacy of dietary supplementation with the spore-forming probiotic strain B. subtilis HU58 in a paediatric population with AAD.
5 Conclusion
The findings of this randomised, double-blind, placebo-controlled trial suggest that B. subtilis HU58 is safe, well-tolerated, and effective at reducing the duration of diarrhoea and associated abdominal pain, and supporting general GI wellbeing, in children with AAD. Future studies should include daily clinical assessment of primary outcomes, validated assessment of abdominal pain and related outcomes, metagenomic and metabolomic assessment of faecal samples and comparison with other probiotics to better understand potential mechanisms underpinning the activity of this specific probiotic strain in AAD.
Corresponding author; e-mail:Â kass@novonesis.com
Acknowledgements
This research was sponsored and funded by Synergia Life Sciences Pvt. Ltd., since acquired by Novozymes A/S (part of the Novonesis group).
Authorsâ contribution
Conceptualisation, SJ; methodology, SJ; validation, SJ; formal analysis, SJ, KS and CH; investigation, PJ and SM; resources, SJ; data curation, KS, CH and SJ; writing â original draft preparation, KS; writing â review and editing, KS, CH and SJ; visualisation, KS and CH; supervision, SJ; project administration, SJ. All authors have read and agreed to the published version of the manuscript.
Conflict of interest
This study was sponsored by Synergia Life Sciences Pvt. Ltd., since acquired by Novozymes A/S (part of the Novonesis group), who manufacture the probiotic strain Bacillus subtilis HU58â¢. Katy Sorensen, Caterina Holz and Shashank Jadhav are employed by entities of the Novonesis group. Pramod Jog and Sanjay Mankar have no conflicts of interest to declare.
References
Agarwal, S., Yewale, V.N. and Dharmapalan, D., 2015. Antibiotics use and misuse in children: a knowledge, attitude and practice survey of parents in India. Journal of Clinical and Diagnostic Research 9: SC21-SC24. https://doi.org/10.7860/jcdr/2015/14933.6819
BauÌ, M., Moretti, A., Bertoni, E., Vazzoler, V., Luini, C., Agosti, M. and Salvatore, S., 2020. Risk and protective factors for gastrointestinal symptoms associated with antibiotic treatment in children: a population study. Pediatric Gastroenterology, Hepatology & Nutrition 23: 35-48. https://doi.org/10.5223/pghn.2020.23.1.35
Binder, H.J., 2010. Role of colonic short-chain fatty acid transport in diarrhea. Annual Review of Physiology 72: 297-313. https://doi.org/10.1146/annurev-physiol-021909-135817
Dhongade, A., Joshi, S., Kulkarni, S., Jadhav, S., Nargundkar, N., Deshmukh, D. and Mehta, A., 2022. The efficacy and safety of a Bacillus probiotic combination for the treatment of acute diarrhea in children: a double-blind, randomized, placebo-controlled multicentric study. The Pediatric Infectious Disease Journal 4: 86-91. https://doi.org/10.5005/jp-journals-10081-1370
Dound, Y.A., Jadhav, S.S., Devale, M., Tom, B., Kiran, K. and Mehta, D.S., 2017. The effect of probiotic Bacillus subtilis HU58 on immune function in healthy human. The Indian Practioner 70: 15-20.
Duysburgh, C., Van Den Abbeele, P., Krishnan, K., Bayne, T.F. and Marzorati, M., 2019. A synbiotic concept containing spore-forming Bacillus strains and a prebiotic fiber blend consistently enhanced metabolic activity by modulation of the gut microbiome in vitro. International Journal of Pharmaceutics: X 1: 1-10. https://doi.org/10.1016/j.ijpx.2019.100021
Endashaw Hareru, H., Sisay, D., Kassaw, C. and Kassa, R., 2022. Antibiotics non-adherence and its associated factors among households in southern Ethiopia. SAGE Open Medicine 10: 1-11. https://doi.org/10.1177/20503121221090472
Francino, M.P., 2015. Antibiotics and the human gut microbiome: dysbioses and accumulation of resistances. Frontiers in Microbiology 6: 1543. https://doi.org/10.3389/fmicb.2015.01543
Gallagher, E.J., Bijur, P.E., Latimer, C. and Silver, W., 2002. Reliability and validity of a visual analog scale for acute abdominal pain in the ED. American Journal of Emerging Medicine 20: 287-290. https://doi.org/10.1053/ajem.2002.33778
Goodman, C., Keating, G., Georgousopoulou, E., Hespe, C. and Levett, K., 2021. Probiotics for the prevention of antibiotic-associated diarrhoea: a systematic review and meta-analysis. BMJ Open 11: e043054. https://doi.org/10.1136/bmjopen-2020-043054
Guo, Q., Goldenberg, J.Z., Humphrey, C., El Dib, R. and Johnston, B.C., 2019. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database of Systematic Reviews 4: CD004827. https://doi.org/10.1002/14651858.CD004827.pub5
Hong, H.A., Khaneja, R., Tam, N.M., Cazzato, A., Tan, S., Urdaci, M., Brisson, A., Gasbarrini, A., Barnes, I. and Cutting, S.M., 2009. Bacillus subtilis isolated from the human gastrointestinal tract. Research in Microbiology 160: 134-143. https://doi.org/10.1016/j.resmic.2008.11.002
Huang, J.M., La Ragione, R.M., Nunez, A. and Cutting, S.M., 2008. Immunostimulatory activity of Bacillus spores. FEMS Immunology and Medical Microbiology 53: 195-203. https://doi.org/10.1111/j.1574-695X.2008.00415.x
Huang, R., Xing, H.Y., Liu, H.J., Chen, Z.F. and Tang, B.B., 2021. Efficacy of probiotics in the treatment of acute diarrhea in children: a systematic review and meta-analysis of clinical trials. Translational Pediatrics 10: 3248-3260. https://doi.org/10.21037/tp-21-511
Karande, S., Sankhe, P. and Kulkarni, M., 2005. Patterns of prescription and drug dispensing. Indian Journal of Pediatrics 72: 117-121. https://doi.org/10.1007/bf02760693
Kotwani, A., Joshi, J., Lamkang, A.S., Sharma, A. and Kaloni, D., 2021. Knowledge and behavior of consumers towards the non-prescription purchase of antibiotics: an insight from a qualitative study from New Delhi, India. Pharmacy Practice 19: 2206. https://doi.org/10.18549/PharmPract.2021.1.2206
Kumar, R., Indira, K., Rizvi, A., Rizvi, T. and Jeyaseelan, L., 2008. Antibiotic prescribing practices in primary and secondary health care facilities in Uttar Pradesh, India. Journal of Clinical Pharmacy and Therapeutics 33: 625-634. https://doi.org/10.1111/j.1365-2710.2008.00960.x
Lewis, S.J. and Heaton, K.W., 1997. Stool form scale as a useful guide to intestinal transit time. Scandinavian Journal of Gastroenterology 32: 920-924. https://doi.org/10.3109/00365529709011203
Mcfarland, L.V., 2008. Antibiotic-associated diarrhea: epidemiology, trends and treatment. Future Microbiology 3: 563-578. https://doi.org/10.2217/17460913.3.5.563
Mehta, A., Brhlikova, P., Mcgettigan, P., Pollock, A.M., Roderick, P. and Farooqui, H.H., 2022. Systemic antibiotic sales and WHO recommendations, India. Bulletin of the World Health Organization 100: 610-619. https://doi.org/10.2471/blt.22.287908
Mehta, D.S., De Souza, A., Jadhav, S. and Devale, M., 2020a. An open labeled, placebo controlled trial to evaluate the role of probiotics-Bacillus subtilis HU58 and Bacillus coagulans SC208 on antibiotic associated diarrhea in humans. Biomedical Journal of Scientific & Technical Research 29: 22679-22684.
Mehta, D.S., De Souza, A., Jadhav, S. and Devale, M., 2020b. A study of probiotic Bacillus subtilis HU58 for the management of antibiotic-associated diarrhoea in adults. The Indian Practitioner 73: 22-28.
Nogrady, B., 2023. The fight against antimicrobial resistance. Nature 624: S30-S32. https://doi.org/10.1038/d41586-023-03912-8.
Porter, J.A., Mackenzie, K.E., Darlow, B.A., Pearson, J.F. and Day, A.S., 2020. A questionnaire-based assessment of gastrointestinal symptoms in children with type 1 diabetes mellitus. Translational Pediatrics 9: 743-749. https://doi.org/10.21037/tp-20-139
Priyadarshini, M., Kotlo, K.U., Dudeja, P.K. and Layden, B.T., 2018. Role of short chain fatty acid receptors in intestinal physiology and pathophysiology. Comprehensive Physiology 8: 1091-1115. https://doi.org/10.1002/cphy.c170050
Rhayat, L., Maresca, M., Nicoletti, C., Perrier, J., Brinch, K.S., Christian, S., Devillard, E. and Eckhardt, E., 2019. Effect of Bacillus subtilis strains on intestinal barrier function and inflammatory response. Frontiers in Immunology 10: 564. https://doi.org/10.3389/fimmu.2019.00564
Singh, R., Sripada, L. and Singh, R., 2014. Side effects of antibiotics during bacterial infection: mitochondria, the main target in host cell. Mitochondrion 16: 50-54. https://doi.org/10.1016/j.mito.2013.10.005
Soares, M.B., Almada, C.N., Pereira, E.P.R., Ferreira, B.M., Balthazar, C.F., Khorshidian, N., Rocha, R.S., Xavier-Santos, D., Cruz, A.G., Ranadheera, C.S., Mortazavian, A.M., GoÌmez-Zavaglia, A., Martinez, R.C.R. and Santâana, A.S., 2023. Review â sporeforming probiotic bacteria: characteristics, health benefits, and technological aspects for their applications in foods and beverages. Trends in Food Science & Technology 138: 453-469.
Wiström, J., Norrby, S.R., Myhre, E.B., Eriksson, S., Granström, G., Lagergren, L., Englund, G., Nord, C.E. and Svenungsson, B., 2001. Frequency of antibiotic-associated diarrhoea in 2462 antibiotic-treated hospitalized patients: a prospective study. Journal of Antimicrobial Chemotherapy 47: 43-50. https://doi.org/10.1093/jac/47.1.43
World Health Organization (WHO), 2001. WHO Global Strategy for Containment of Antimicrobial Resistance. Available from: https://iris.who.int/bitstream/handle/10665/66860/WHO_CDS_CSR_DRS_2001.2.pdf?sequence=1
Yang, Q., Hu, Z., Lei, Y., Li, X., Xu, C., Zhang, J., Liu, H. and Du, X., 2023. Overview of systematic reviews of probiotics in the prevention and treatment of antibiotic-associated diarrhea in children. Front Pharmacol 14: 1-15. https://doi.org/10.3389/fphar.2023.1153070


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}