Abstract
Clinical guidelines are recommendations for healthcare providers regarding patients with specific conditions. These guidelines should be based on practice experience and the best available research evidence. However, guidelines developed by various health organisations worldwide often do not agree with each other. This is also true for the current guidelines for the clinical use of probiotics. This article aims to provide examples of conflicting clinical guidelines for probiotics, define reasons for this phenomenon, describe standard tools for improving their quality, and suggest ways to enhance the development and assessment of suitable clinical guidelines for the appropriate clinical use of probiotics in specific conditions.
1 Introduction
The number of clinical guidelines and recommendations has expanded dramatically over the past few decades, and parallel efforts have been made to standardise their development and ensure their quality. Such guidelines play an important role in improving the quality and value of healthcare by synthesising large amounts of evidence to provide standardised recommendations to healthcare professionals and patients (Kredo et al., 2016). Clinical guidelines are intended to provide systematic aid for making complex medical decisions. When rigorously developed using a transparent process that combines scientific evidence based on randomised controlled trials (RCT), clinician experiential knowledge, and patient values, they can improve many clinician and patient healthcare decisions and enhance healthcare quality and outcomes. Imperfect clinical guidelines can harm healthcare professionals by providing inaccurate scientific information and clinical advice, compromising care quality. Their growing influence has also increased concern for potential sources of bias. Conflicting guidelines from different professional bodies can also confuse and frustrate practitioners. Guidelines and recommendations for the clinical use of probiotics suffer from similar problems. This document aims to provide examples of conflicting clinical guidelines for probiotics, define reasons for this phenomenon, and suggest ways to improve the development and assessment of suitable clinical guidelines for the appropriate clinical use of probiotics.
2 Examples of conflicting guidelines
We present two examples of contradictory guidelines regarding the use of probiotics in clinical settings. These examples are from the field of gastroenterology. The first example asks whether to use probiotics to manage acute gastroenteritis (AGE). Until 2019, most professional societies and groups of experts have advocated the use of probiotics to manage this disorder. In 2020, conflicting recommendations appeared in the medical literature.
On the one hand, the American Gastroenterology Association (AGA) recommended that this therapeutic tool not be used in AGE (Su et al., 2020). At the same time, the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) supported using a few particular probiotic strains (Szajewska et al., 2020). In 2021, an additional network meta-analysis from China, based on a single RCT, endorsed the use of probiotics, with a few differences from the previous recommendations (Su et al., 2020).
An additional example is the use of probiotics in preventing Clostridium difficile infections, primary and recurrent. The AGA supported using four specific strains of probiotics based on several meta-analyses accounting for strain specificity (Su et al., 2020). A year later, the American College of Gastroenterology (ACG) was against the use of probiotics in this situation, based on only one underpowered RCT and several meta-analyses pooling data of different strains without accounting for strain specificity. The recommendation was to use fecal microbiota transplantation instead (Kelly et al., 2021). The differing conclusions of these two examples highlight the effect of applying different types of evidence to evaluate distinct interventions and the impact of not accounting for probiotic strain specificity.

Reasons for conflicting guidelines
Citation: Beneficial Microbes 15, 4 (2024) ; 10.1163/18762891-bja00027
3 Reasons for conflicting guidelines
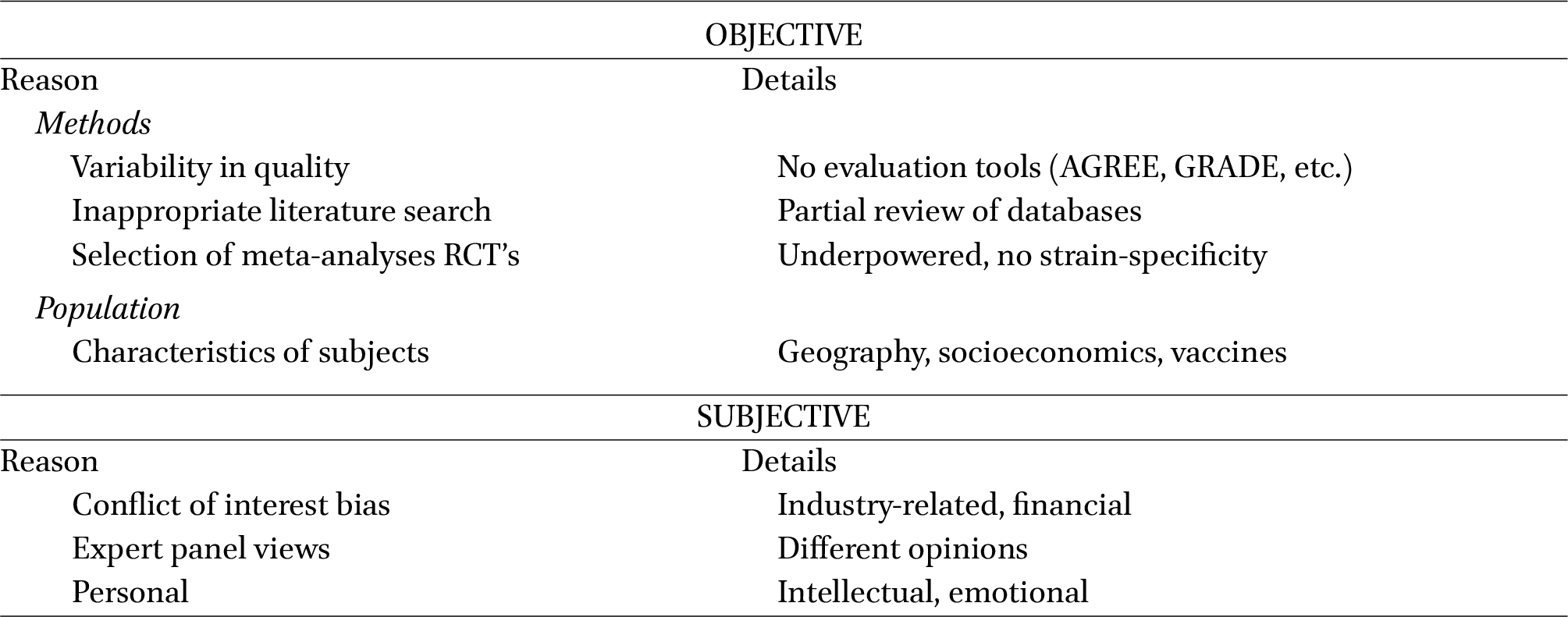
There are various reasons why guidelines can sometimes conflict. An analysis of such reasons is presented in Table 1. Objective reasons concerning the methodology include imperfect quality due to a lack of evaluation tools such as the AGREE and GRADE methods (Brouwers et al., 2010a; Guyatt et al., 2008). Details of such methods are described in the next section. An incomplete literature search of the standard databases, such as Medline, Embase, Cochrane, Dare, and CENTRAL, is an additional cause. Appropriate recommendations should be based on more than just a single RCT but rather on suitable meta-analyses based on reliable RCTs that are not underpowered and account for strain specificity. Additional objective factors include diverse population characteristics, such as socioeconomic levels, medical issues, vaccination, and geographical features.
A major subjective factor among guideline developers is the conflict-of-interest (COI) bias. In a survey of 100 authors across 37 guidelines, 87% had a financial relationship with the industry and 59% with companies whose products were considered in a guideline. Of the 59%, 64% received speaking honorariums, and 38% were company employees or consultants (Choudhry et al., 2002).
In a comparison of two Hematology societies, where 73% reported an association with pharmaceutical companies, more experts gave a stronger recommendation for agents manufactured by those companies (George et al., 2014). In a cross-sectional survey of 95 national and international medical organisations that produced 290 clinical practice guidelines, 63% reported receiving funds from a biomedical company (Campsall et al., 2016). There is a need for an effective policy to manage organisational COI and disclosure of the financial relationship.
Additional causes include diverse views among expert panel members and varied personality characteristics.
A recent analysis studied inappropriate discordant recommendations by comparing consensus-based and evidence-based guidelines. The guidelines were created by the American College of Cardiology, the American Heart Association, and the American Society of Clinical Oncology until March 2021. A total of 81 guidelines were found, producing 2,528 recommendations. Consensus-based methods resulted in 2.6 to 5.1 times greater odds of issuing inappropriate discordant recommendations than evidence-based methods. The study’s authors suggest that all guidelines should be evidence-based, and organisations should prioritise avoiding inappropriate discordant recommendations (Yao et al., 2021).
Tools for the development and evaluation of guidelines
Citation: Beneficial Microbes 15, 4 (2024) ; 10.1163/18762891-bja00027
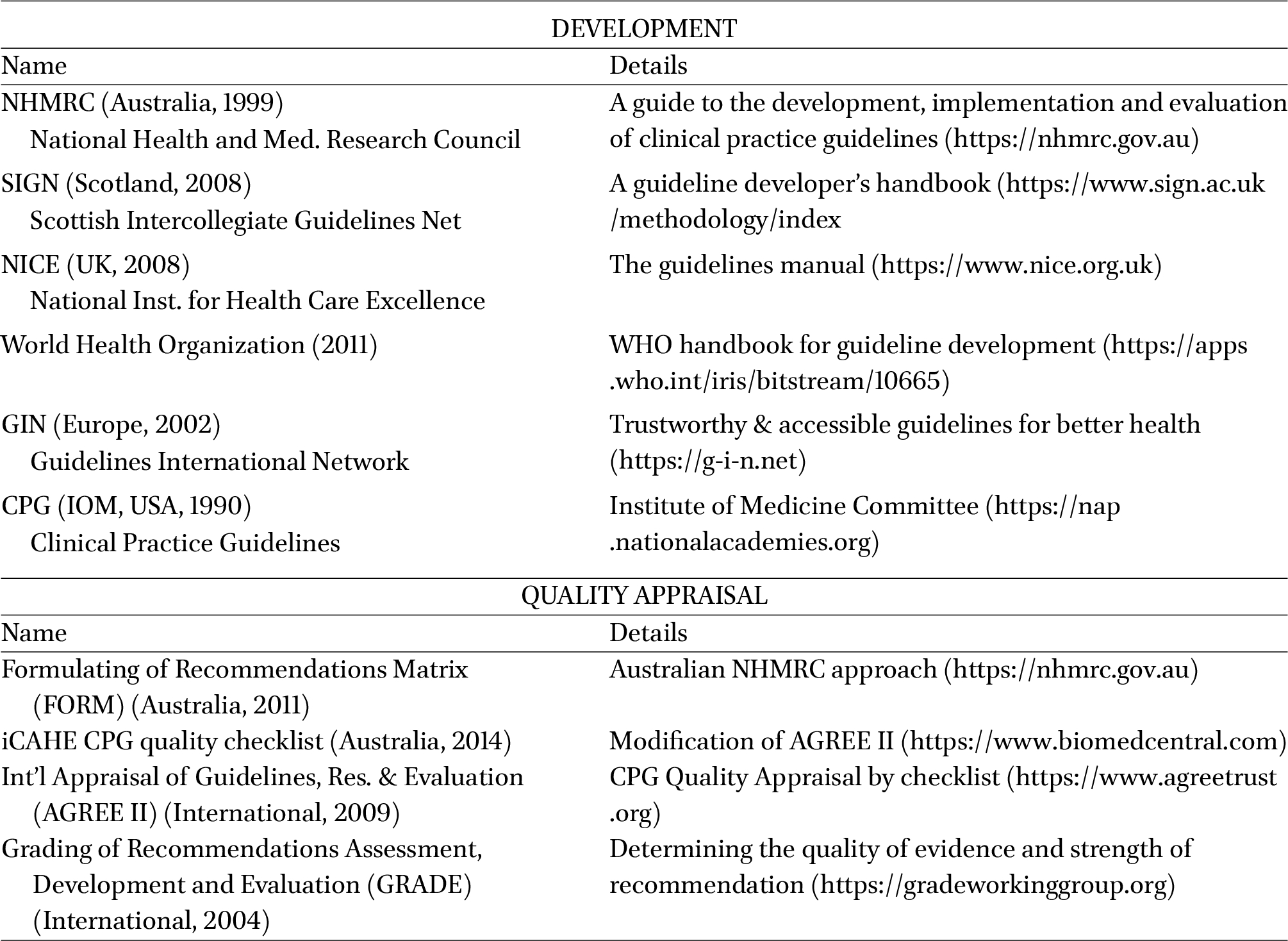
4 Tools for the development and evaluation of guidelines
A description of various tools for developing and evaluating guidelines is presented in Table 2. We will focus only on the significant tools that this document recommends. One of the most common and widely used approach has been developed by the American Institute of Medicine (IOM) since 1990. They define clinical practice guidelines (CPG) as ‘statements that include recommendations intended to optimise patient care, that are informed by a systematic review of evidence and an assessment of the benefits and harms of alternative care options’. In addition, the IOM also defined standards for developing trustworthy CPGs. It includes eight elements: transparency, conflict of interest, members of the guidelines development group, literature review, rating the strength of evidence and recommendations, presentation of recommendations, external review, and updating (Kredo et al., 2016).
The AGREE II has become an internationally accepted standard for evaluating the methodological quality of CPGs. Its items and criteria have been reformatted to create a reporting guide called the AGREE Reporting Checklist. This checklist is intended to improve the comprehensiveness, completeness, and transparency of reporting in CPGs. It consists of six domains, 23 items, and two global rating items, each scored 1-7 (Brouwers et al., 2010b).
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system is an additional tool for determining the quality of evidence and strength of recommendation. It consists of four categories for the quality of the evidence and two categories for the strength of recommendation. It’s the most widely adopted tool and is endorsed by over 100 organisations worldwide (Guyatt et al., 2008).
The Delphi method is a systematic process to measure and develop consensus among members of an expert group. It aims to determine the extent to which experts agree about a particular issue, with the ultimate goal of providing a unified specialist opinion. This structured process uses a series of questionnaires or ‘rounds’ to gather information. Rounds are held until group consensus is reached (Boulkedid et al., 2011).
5 Proposal
Our review discloses that conflicting guidelines for probiotics are not rare. Most of them are due to poor methodology and conflict of interest issues. Many practical tools exist for developing trustworthy guidelines. Guidelines for the clinical use of ‘Biotics’ (probiotics, prebiotics, synbiotics, and postbiotics) should be developed and evaluated based on the above reliable techniques. We suggest implementing the following steps:
- 1. A comprehensive electronic search of databases is preferable.
- 2. It is vital to select meta-analyses based on reliable RCTs that are not underpowered and that account for strain specificity. Avoid basing a recommendation on a single trial.
- 3. To develop trustworthy CPG, using the American IOM elements is essential.
- 4. Including the AGREE II system for the CPG Quality Appraisal by a checklist is needed.
- 5. The GRADE system should be adopted to evaluate the quality of evidence and strength of recommendations.
- 6. The addition of the Delphi process to establish expert group consensus on statements is suggested.
Healthcare organisations worldwide that deal with probiotics, such as the International Probiotics Association (IPA) and the International Scientific Association for Probiotics and Prebiotics (ISAPP), should adopt these tools and implement and encourage their use. Developing high-quality guidelines for ‘Biotics’ is critical to improving physicians’ decision-making and patient outcomes.
Corresponding author; e-mail: wzvi@bgu.ac.il
Authors’ contribution
Concept and writing of the manuscript: ZW, corrections, and editing: YV. Both authors read and approved the final manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
No external funding was received for this manuscript.
References
Boulkedid, R., Abdoul, H., Loustau, M., Sibony, O. and Alberti, C., 2011. Using and reporting the Delphi method for selecting healthcare quality indicators: a systematic review. PLoS One 6: e20476. https://doi.org/10.1371/journal.pone.0020476
Brouwers, M.C., Kho, M.E., Browman, G.P., Burgers, J.S., Cluzeau, F., Feder, G., Fervers, B., Graham, I.D., Hanna, S.E., Makarski, J. and the Agree Next Steps Consortium, 2010a. Development of the AGREE II, part 1: performance, usefulness and areas for improvement. Canadian Medical Association Journal 182: 1045-1052. https://doi.org/10.1503/cmaj.091714
Brouwers, M.C., Kho, M.E., Browman, G.P., Burgers, J.S., Cluzeau, F., Feder, G., Fervers, B., Graham, I.D., Hanna, S.E., Makarski, J. and the Agree Next Steps Consortium, 2010b. Development of the AGREE II, part 2: assessment of validity of items and tools to support application. Canadian Medical Association Journal 182: E472-E478. https://doi.org/10.1503/cmaj.091716
Campsall, P., Colizza, K., Straus, S. and Stelfox, H.T., 2016. Financial relationships between organizations that produce clinical practice guidelines and the biomedical industry: a cross-sectional study. PLoS Medicine 13: e1002029. https://doi.org/10.1371/journal.pmed.1002029
Choudhry, N.K., Stelfox, H.T. and Detsky, A.S., 2002. Relationships between authors of clinical practice guidelines and the pharmaceutical industry. JAMA 287: 612-617. https://doi.org/10.1001/jama.287.5.612
George, J.N., Vesely, S.K. and Woolf, S.H., 2014. Conflicts of interest and clinical recommendations: comparison of two concurrent clinical practice guidelines for primary immune thrombocytopenia developed by different methods. American Journal of Medical Quality 29: 53-60. https://doi.org/10.1177/1062860613481618
Guyatt, G.H., Oxman, A.D., Vist, G.E., Kunz, R., Falck-Ytter, Y., Alonso-Coello, P., Schunemann, H.J. and the GRADE Working Group, 2008. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336: 924-926. https://doi.org/10.1136/bmj.39489.470347.AD
Kelly, C.R., Fischer, M., Allegretti, J.R., LaPlante, K., Stewart, D.B., Limketkai, B.N. and Stollman, N.H., 2021. ACG clinical guidelines: prevention, diagnosis, and treatment of Clostridioides difficile infections. American Journal of Gastroenterology 116: 1124-1147. https://doi.org/10.14309/ajg.0000000000001278
Kredo, T., Bernhardsson, S., Machingaidze, S., Young, T., Louw, Q., Ochodo, E. and Grimmer, K., 2016. Guide to clinical practice guidelines: the current state of play. International Journal for Quality in Health Care 28: 122-128. https://doi.org/10.1093/intqhc/mzv115
Su, G.L., Ko, C.W., Bercik, P., Falck-Ytter, Y., Sultan, S., Weizman, A.V. and Morgan, R.L., 2020. AGA clinical practice guidelines on the role of probiotics in the management of gastrointestinal disorders. Gastroenterology 159: 697-705. https://doi.org/10.1053/j.gastro.2020.05.059
Szajewska, H., Guarino, A., Hojsak, I., Indrio, F., Kolacek, S., Orel, R., Salvatore, S., Shamir, R., van Goudoever, J.B., Vandenplas, Y., Weizman, Z., Zalewski, B.M. and on behalf of the Working Group on Probiotics and Prebiotics of the European Society for Paediatric Gastroenterology, Hepatology and Nutrition, 2020. Use of probiotics for the management of acute gastroenteritis in children: an update. Journal of Pediatric Gastroenterology and Nutrition 71: 261-269. https://doi.org/10.1097/MPG.0000000000002751
Yao, L., Ahmed, M.M., Guyatt, G.H., Yan, P., Hui, X., Wang, Q., Yang, K., Tian, J. and Djulbegovic, B., 2021. Discordant and inappropriate discordant recommendations in consensus and evidence based guidelines: empirical analysis. BMJ 375: e066045. https://doi.org/10.1136/bmj-2021-066045

{kind=link}
{kind=link}